

Personalized virtual-heart technology for guiding the ablation of infarct-related ventricular tachycardia
- PMID: 30847259
- PMCID: PMC6400313
- DOI: 10.1038/s41551-018-0282-2
Personalized virtual-heart technology for guiding the ablation of infarct-related ventricular tachycardia
Abstract
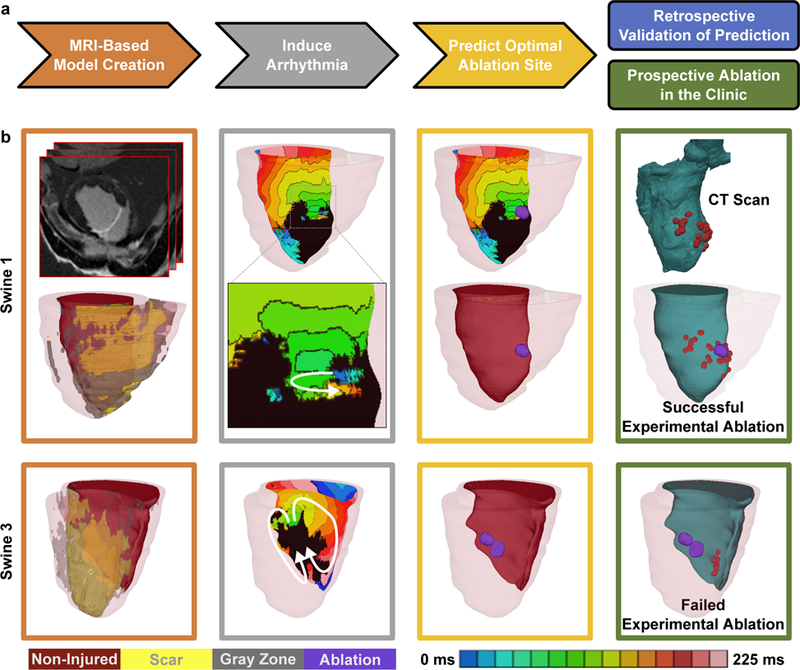
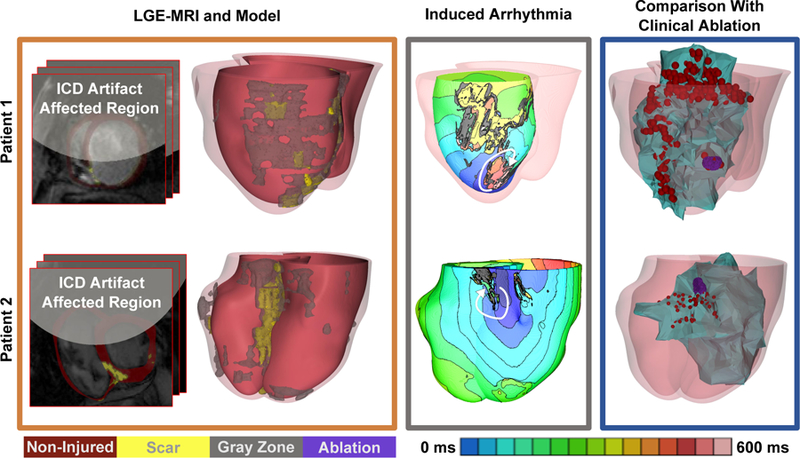
Ventricular tachycardia (VT), which can lead to sudden cardiac death, occurs frequently in patients with myocardial infarction. Catheter-based radiofrequency ablation of cardiac tissue has achieved only modest efficacy, owing to the inaccurate identification of ablation targets by current electrical mapping techniques, which can lead to extensive lesions and to a prolonged, poorly tolerated procedure. Here we show that personalized virtual-heart technology based on cardiac imaging and computational modelling can identify optimal infarct-related VT ablation targets in retrospective animal (5 swine) and human studies (21 patients) and in a prospective feasibility study (5 patients). We first assessed in retrospective studies (one of which included a proportion of clinical images with artifacts) the capability of the technology to determine the minimum-size ablation targets for eradicating all VTs. In the prospective study, VT sites predicted by the technology were targeted directly, without relying on prior electrical mapping. The approach could improve infarct-related VT ablation guidance, where accurate identification of patient-specific optimal targets could be achieved on a personalized virtual heart prior to the clinical procedure.
Conflict of interest statement
Competing Interests. NAT holds partial ownership of CardioSolv Ablation Technologies LLC. SN is a scientific advisor to CardioSolv Ablation Technologies LLC. The other authors declare no competing financial and non-financial interests.
Figures


Comment in
-
3D virtual heart to guide VT ablation.Nat Rev Cardiol. 2018 Nov;15(11):654. doi: 10.1038/s41569-018-0102-0. Nat Rev Cardiol. 2018. PMID: 30258133 No abstract available.
-
Virtual heart guides cardiac ablation.Nat Biomed Eng. 2018 Oct;2(10):711-712. doi: 10.1038/s41551-018-0303-1. Nat Biomed Eng. 2018. PMID: 31015644 No abstract available.
References
-
- Stevenson WG et al. Radiofrequency catheter ablation of ventricular tachycardia after myocardial infarction. Circulation 98, 308–314 (1998). - PubMed
-
- Brugada J et al. Nonsurgical transthoracic epicardial radiofrequency ablation: an alternative in incessant ventricular tachycardia. J Am Coll Cardiol 41, 2036–2043 (2003). - PubMed
-
- Sosa E, Scanavacca M, d’Avila A, Oliveira F & Ramires JA Nonsurgical transthoracic epicardial catheter ablation to treat recurrent ventricular tachycardia occurring late after myocardial infarction. J Am Coll Cardiol 35, 1442–1449 (2000). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
