

Low-Dose vs. High-Dose Cisplatin: Lessons Learned From 59 Chemoradiotherapy Trials in Head and Neck Cancer
- PMID: 30847300
- PMCID: PMC6394212
- DOI: 10.3389/fonc.2019.00086
Low-Dose vs. High-Dose Cisplatin: Lessons Learned From 59 Chemoradiotherapy Trials in Head and Neck Cancer
Abstract
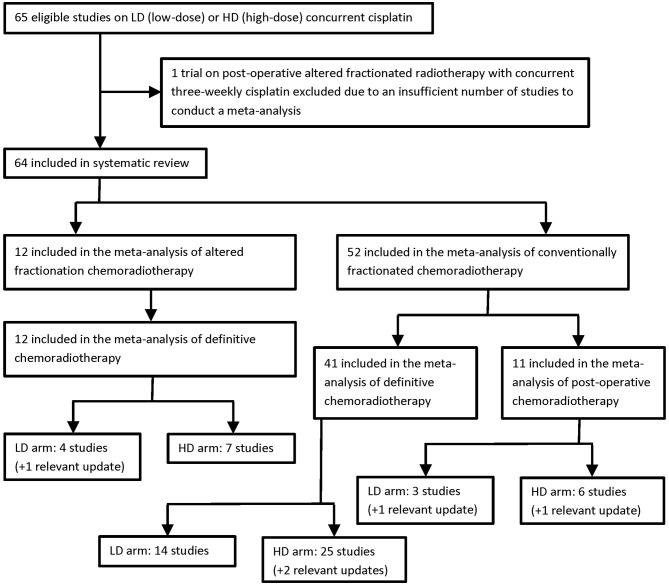
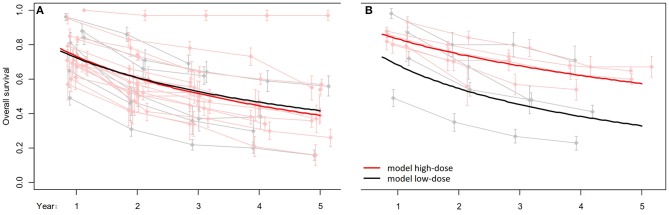
In locally advanced squamous cell carcinomas of the head and neck (LA-SCCHN), concurrent chemoradiotherapy is an integral part of multimodality management both in the adjuvant and in the definitive settings. Although de-intensification strategies have been propelled to the forefront of clinical research in human papillomavirus (HPV) positive oropharyngeal cancer, three cycles of 100 mg/m2 cisplatin given every 3 weeks concurrently with conventionally fractionated external beam radiotherapy represent a cost-effective and globally accessible treatment option for the majority of LA-SCCHN cases. Based on four large randomized trials, this regimen has become the non-surgical standard of care for cisplatin-eligible patients. Nevertheless, the outcomes in terms of efficacy, toxicity, and compliance have been rather disappointing. Therefore, there is an unmet need to find a better alternative. With limited support from randomized trials, weekly low-dose cisplatin regimens have replaced the standard high-dose schedule at some institutions. Four prospective trials exploring radiotherapy with and without weekly low-dose cisplatin have been published. Two of them were conducted in the 1980s, one of which had a negative outcome, the third study provided insufficient information on toxicity, and the fourth trial had to be prematurely terminated due to poor accrual. Moreover, the findings of two phase III trials comparing the two concurrent cisplatin regimens favored the high-dose protocol. We performed a composite meta-analysis of 59 prospective trials enrolling a total of 5,582 patients. The primary endpoint was overall survival. Reflecting different radiotherapy fractionation schemes and treatment intents, three meta-analyses were carried out, one for postoperative conventional chemoradiotherapy, one for definitive conventional chemoradiotherapy, and one for definitive altered fractionation chemoradiotherapy. In the former two settings, both high- and low-dose regimens yielded similar survival outcomes, thus, the primary objective was not met. When given concurrently with altered fractionation radiotherapy, patients treated with high-dose cisplatin had significantly longer overall survival than those who received low-dose cisplatin. In this article we provide a synthetic view of the results, discuss the issue of cumulative dose, compare two vs. three cycles of high-dose cisplatin, and present our three-step recommendations for use of the current standard of care, high-dose cisplatin, in clinical practice.
Keywords: chemoradiotherapy; cisplatin; clinical trials; cumulative dose; fractionation; head and neck cancer; practice recommendations.
Figures
Similar articles
-
Altered fractionation radiotherapy combined with concurrent low-dose or high-dose cisplatin in head and neck cancer: A systematic review of literature and meta-analysis.Oral Oncol. 2018 Jan;76:52-60. doi: 10.1016/j.oraloncology.2017.11.025. Epub 2017 Dec 8. Oral Oncol. 2018. PMID: 29290286
-
Phase II/III Randomized Controlled Trial of Concomitant Hyperfractionated Radiotherapy plus Cetuximab (Anti-EGFR Antibody) or Chemotherapy in Locally Advanced Head and Neck Cancer.Gulf J Oncolog. 2019 May;1(30):6-12. Gulf J Oncolog. 2019. PMID: 31242976 Clinical Trial.
-
Concurrent chemoradiotherapy with cisplatin given once-a-week versus every-three weekly in head and neck squamous cell carcinoma: Non-inferior, equivalent, or superior?Oral Oncol. 2022 Nov;134:106130. doi: 10.1016/j.oraloncology.2022.106130. Epub 2022 Sep 24. Oral Oncol. 2022. PMID: 36162191
-
Concomitant adjuvant chemoradiotherapy with weekly low-dose cisplatin for high-risk squamous cell carcinoma of the head and neck: a phase II prospective trial.Clin Oncol (R Coll Radiol). 2011 Mar;23(2):134-40. doi: 10.1016/j.clon.2010.09.004. Epub 2010 Oct 27. Clin Oncol (R Coll Radiol). 2011. PMID: 21030225 Clinical Trial.
-
Cisplatin Eligibility Issues and Alternative Regimens in Locoregionally Advanced Head and Neck Cancer: Recommendations for Clinical Practice.Front Oncol. 2019 Jun 11;9:464. doi: 10.3389/fonc.2019.00464. eCollection 2019. Front Oncol. 2019. PMID: 31245288 Free PMC article. Review.
Cited by
-
Genes Regulated by HPV 16 E6 and High Expression of NFX1-123 in Cervical Cancers.Onco Targets Ther. 2020 Jun 26;13:6143-6156. doi: 10.2147/OTT.S251926. eCollection 2020. Onco Targets Ther. 2020. PMID: 32617009 Free PMC article.
-
Mechanisms of Cisplatin-Induced Acute Kidney Injury: Pathological Mechanisms, Pharmacological Interventions, and Genetic Mitigations.Cancers (Basel). 2021 Mar 29;13(7):1572. doi: 10.3390/cancers13071572. Cancers (Basel). 2021. PMID: 33805488 Free PMC article. Review.
-
The Role and Efficacy of JNK Inhibition in Inducing Lung Cancer Cell Death Depend on the Concentration of Cisplatin.ACS Omega. 2024 Jun 18;9(26):28311-28322. doi: 10.1021/acsomega.4c01950. eCollection 2024 Jul 2. ACS Omega. 2024. PMID: 38973918 Free PMC article.
-
Best Practice in Systemic Therapy for Head and Neck Squamous Cell Carcinoma.Front Oncol. 2019 Aug 27;9:815. doi: 10.3389/fonc.2019.00815. eCollection 2019. Front Oncol. 2019. PMID: 31508372 Free PMC article. Review.
-
Utility of Prophylactic Percutaneous Gastrostomy in Patients With Head and Neck Cancer Receiving Concurrent Chemoradiotherapy: A Multicenter Analysis.Cureus. 2023 Sep 4;15(9):e44637. doi: 10.7759/cureus.44637. eCollection 2023 Sep. Cureus. 2023. PMID: 37671078 Free PMC article.
References
-
- Noone AM, Howlader N, Krapcho M, Miller D, Brest A, Yu M, et al. (eds.). SEER Cancer Statistics Review, 1975-2015, Bethesda, MD: National Cancer Institute; (2018). Available online at: https://seer.cancer.gov/csr/1975_2015/, based on November 2017 SEER data submission, posted to the SEER web site.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous