

Adjusting for social risk factors impacts performance and penalties in the hospital readmissions reduction program
- PMID: 30848491
- PMCID: PMC6407348
- DOI: 10.1111/1475-6773.13133
Adjusting for social risk factors impacts performance and penalties in the hospital readmissions reduction program
Abstract
Objective: Medicare's Hospital Readmissions Reduction Program (HRRP) does not account for social risk factors in risk adjustment, and this may lead the program to unfairly penalize safety-net hospitals. Our objective was to determine the impact of adjusting for social risk factors on HRRP penalties.
Study design: Retrospective cohort study.
Data sources/study setting: Claims data for 2 952 605 fee-for-service Medicare beneficiaries with acute myocardial infarction (AMI), congestive heart failure (CHF) or pneumonia from December 2012 to November 2015.
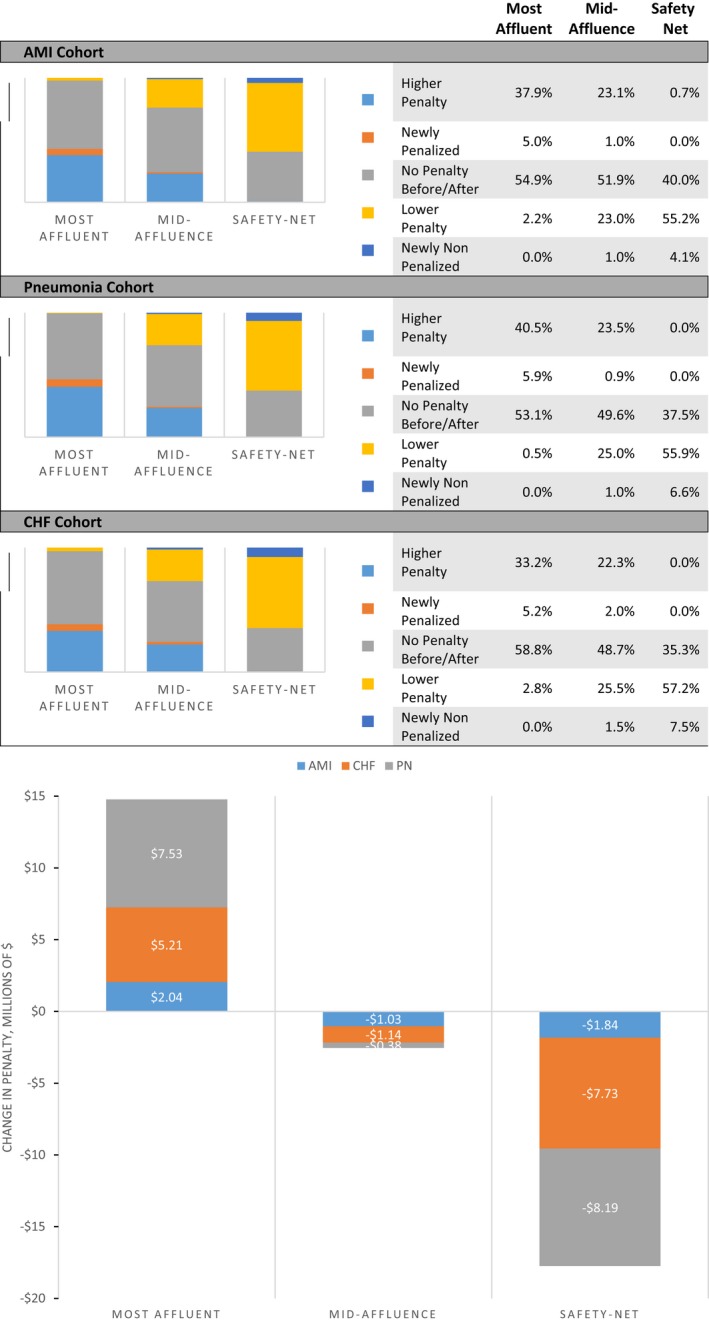
Principal findings: Poverty, disability, housing instability, residence in a disadvantaged neighborhood, and hospital population from a disadvantaged neighborhood were associated with higher readmission rates. Under current program specifications, safety-net hospitals had higher readmission ratios (AMI, 1.020 vs 0.986 for the most affluent hospitals; pneumonia, 1.031 vs 0.984; and CHF, 1.037 vs 0.977). Adding social factors to risk adjustment cut these differences in half. Over half the safety-net hospitals saw their penalty decline; 4-7.5 percent went from having a penalty to having no penalty. These changes translated into a $17 million reduction in penalties to safety-net hospitals.
Conclusions: Accounting for social risk can have a major financial impact on safety-net hospitals. Adjustment for these factors could reduce negative unintended consequences of the HRRP.
Keywords: Medicare; readmission.
© Health Research and Educational Trust.
Conflict of interest statement
Dr. Joynt Maddox does intermittent contract work for the United States Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Dr. Kind receives grant funding from the NIH/National Institute on Minority Health and Health Disparities, the NIH/National Institute on Aging, the Commonwealth Fund, the US Department of Veterans Affairs, and the US Centers for Medicare and Medicaid Services, and has performed work as a consultant for the US state of Maryland. Dr. Zaslavsky receives support under grants and contracts from the National Institutes on Aging and on Mental Health, and from the Centers for Medicare and Medicaid Services. Mr. Reidhead, Dr. Nerenz, Dr. Nagasako, and Dr. Hu report no conflicts.
Figures
Similar articles
-
Changes to Racial Disparities in Readmission Rates After Medicare's Hospital Readmissions Reduction Program Within Safety-Net and Non-Safety-Net Hospitals.JAMA Netw Open. 2018 Nov 2;1(7):e184154. doi: 10.1001/jamanetworkopen.2018.4154. JAMA Netw Open. 2018. PMID: 30646342 Free PMC article.
-
Association Between Hospital Penalty Status Under the Hospital Readmission Reduction Program and Readmission Rates for Target and Nontarget Conditions.JAMA. 2016 Dec 27;316(24):2647-2656. doi: 10.1001/jama.2016.18533. JAMA. 2016. PMID: 28027367 Free PMC article.
-
Readmissions performance and penalty experience of safety-net hospitals under Medicare's Hospital Readmissions Reduction Program.BMC Health Serv Res. 2022 Mar 15;22(1):338. doi: 10.1186/s12913-022-07741-9. BMC Health Serv Res. 2022. PMID: 35287693 Free PMC article.
-
Hospital readmissions reduction program penalizes safety net hospital clinicians.JAAPA. 2024 Dec 1;37(12):44-47. doi: 10.1097/01.JAA.0000000000000161. Epub 2024 Dec 21. JAAPA. 2024. PMID: 39569857
-
Social Risk Adjustment In The Hospital Readmissions Reduction Program: A Systematic Review And Implications For Policy.Health Aff (Millwood). 2022 Sep;41(9):1307-1315. doi: 10.1377/hlthaff.2022.00614. Health Aff (Millwood). 2022. PMID: 36067432 Free PMC article.
Cited by
-
Exit Rates of Accountable Care Organizations That Serve High Proportions of Beneficiaries of Racial and Ethnic Minority Groups.JAMA Health Forum. 2022 Sep 2;3(9):e223398. doi: 10.1001/jamahealthforum.2022.3398. JAMA Health Forum. 2022. PMID: 36218951 Free PMC article.
-
Evaluating How Safety-Net Hospitals Are Identified: Systematic Review and Recommendations.Health Equity. 2022 Apr 14;6(1):298-306. doi: 10.1089/heq.2021.0076. eCollection 2022. Health Equity. 2022. PMID: 35557553 Free PMC article. Review.
-
Racial, Ethnic, and Socioeconomic Disparities in Access to Transcatheter Aortic Valve Replacement Within Major Metropolitan Areas.JAMA Cardiol. 2022 Feb 1;7(2):150-157. doi: 10.1001/jamacardio.2021.4641. JAMA Cardiol. 2022. PMID: 34787635 Free PMC article.
-
Neighborhood Socioeconomic Disadvantage and Mortality Among Medicare Beneficiaries Hospitalized for Acute Myocardial Infarction, Heart Failure, and Pneumonia.J Gen Intern Med. 2022 Jun;37(8):1894-1901. doi: 10.1007/s11606-021-07090-z. Epub 2021 Sep 10. J Gen Intern Med. 2022. PMID: 34505979 Free PMC article.
-
Nursing Home Alzheimer's Special Care Units: Geographic Location Matters.J Am Med Dir Assoc. 2022 Jan;23(1):150-155. doi: 10.1016/j.jamda.2021.07.020. Epub 2021 Aug 17. J Am Med Dir Assoc. 2022. PMID: 34411539 Free PMC article.
References
-
- Joynt KE, Jha AK. Thirty‐day readmissions–truth and consequences. N Engl J Med. 2012;366(15):1366‐1369. - PubMed
-
- Joynt Maddox KE, Chen LM, Zuckerman R, Epstein AM. Association between race, neighborhood, and medicaid enrollment and outcomes in medicare home health care. J Am Geriatr Soc. 2018;66(2):239‐246. - PubMed
-
- Hu J, Gonsahn MD, Nerenz DR. Socioeconomic status and readmissions: evidence from an urban teaching hospital. Health Aff (Millwood). 2014;33(5):778‐785. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
