

Treatment to Target Using Recombinant Interleukin-1 Receptor Antagonist as First-Line Monotherapy in New-Onset Systemic Juvenile Idiopathic Arthritis: Results From a Five-Year Follow-Up Study
- PMID: 30848528
- PMCID: PMC6617757
- DOI: 10.1002/art.40865
Treatment to Target Using Recombinant Interleukin-1 Receptor Antagonist as First-Line Monotherapy in New-Onset Systemic Juvenile Idiopathic Arthritis: Results From a Five-Year Follow-Up Study
Abstract
Objective: Systemic juvenile idiopathic arthritis (JIA) is a multifactorial autoinflammatory disease with a historically poor prognosis. With current treatment regimens, approximately half of patients still experience active disease after 1 year of therapy. This study was undertaken to evaluate a treat-to-target approach using recombinant interleukin-1 receptor antagonist (rIL-1Ra; anakinra) as first-line monotherapy to achieve early inactive disease and prevent damage.
Methods: In this single-center, prospective study, patients with new-onset systemic JIA with an unsatisfactory response to nonsteroidal antiinflammatory drugs received rIL-1Ra monotherapy according to a treat-to-target strategy. Patients with an incomplete response to 2 mg/kg rIL-1Ra subsequently received 4 mg/kg rIL-1Ra or additional prednisolone, or switched to alternative therapy. For patients in whom inactive disease was achieved, rIL-1Ra was tapered after 3 months and subsequently stopped.
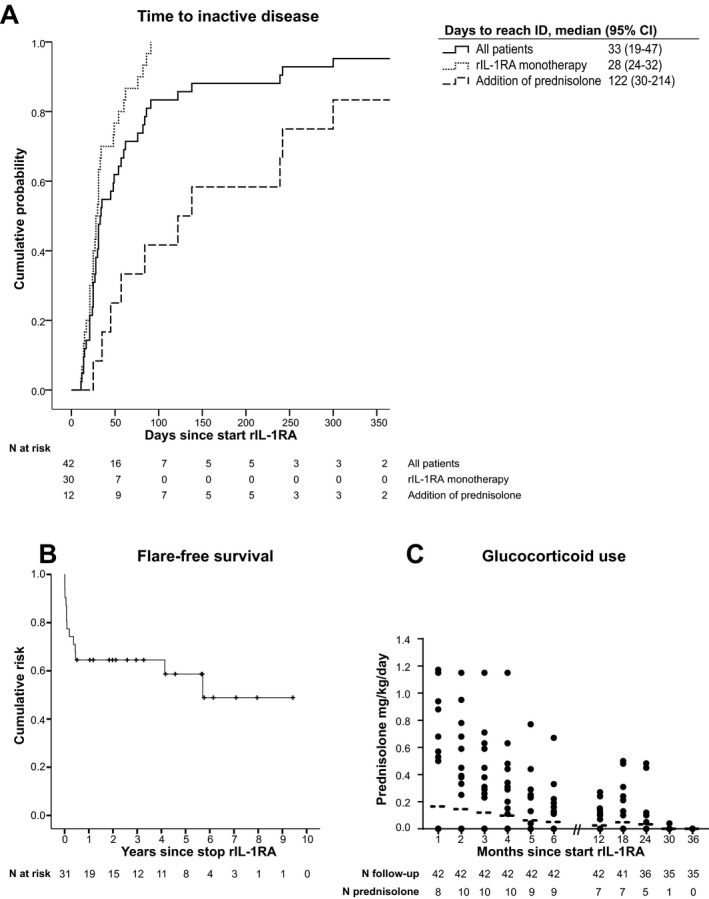
Results: Forty-two patients, including 12 who had no arthritis at disease onset, were followed up for a median of 5.8 years. The median time to achieve inactive disease was 33 days. At 1 year, 76% had inactive disease, and 52% had inactive disease while not receiving medication. High neutrophil counts at baseline and a complete response after 1 month of rIL-1Ra were highly associated with inactive disease at 1 year. After 5 years of follow-up, 96% of the patients included had inactive disease, and 75% had inactive disease while not receiving medication. Articular or extraarticular damage was reported in <5%, and only 33% of the patients received glucocorticoids. Treatment with rIL-1Ra was equally effective in systemic JIA patients without arthritis at disease onset.
Conclusion: Treatment to target, starting with first-line, short-course monotherapy with rIL-1Ra, is a highly efficacious strategy to induce and sustain inactive disease and to prevent disease- and glucocorticoid-related damage in systemic JIA.
© 2019 The Authors. Arthritis & Rheumatology published by Wiley Periodicals, Inc. on behalf of American College of Rheumatology.
Figures


Comment in
-
A Bullseye for Children With Systemic Juvenile Idiopathic Arthritis.Arthritis Rheumatol. 2019 Jul;71(7):1030-1033. doi: 10.1002/art.40867. Epub 2019 May 27. Arthritis Rheumatol. 2019. PMID: 30802004 Free PMC article. No abstract available.
References
-
- Petty RE, Southwood TR, Manners P, Baum J, Glass DN, Goldenberg J, et al. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol 2004;31:390–2. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
