

Race/Ethnicity and Geographic Access to Urban Trauma Care
- PMID: 30848804
- PMCID: PMC6484639
- DOI: 10.1001/jamanetworkopen.2019.0138
Race/Ethnicity and Geographic Access to Urban Trauma Care
Abstract
Importance: Little is known about the distribution of life-saving trauma resources by racial/ethnic composition in US cities, and if racial/ethnic minority populations disproportionately live in US urban trauma deserts.
Objective: To examine racial/ethnic differences in geographic access to trauma care in the 3 largest US cities, considering the role of residential segregation and neighborhood poverty.
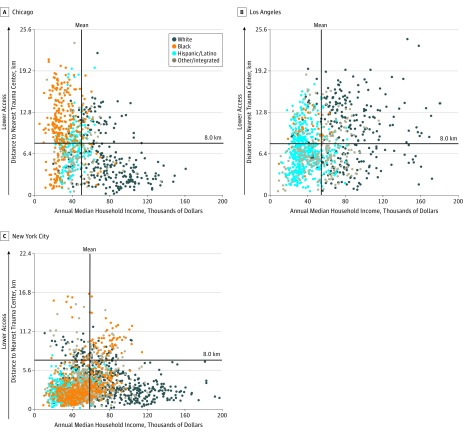
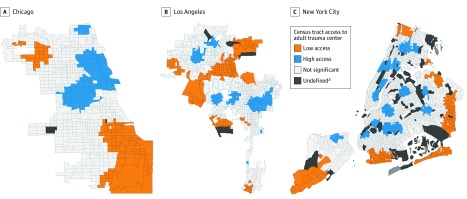
Design, setting, and participants: A cross-sectional, multiple-methods study evaluated census tract data from the 2015 American Community Survey in Chicago, Illinois; Los Angeles (LA), California; and New York City (NYC), New York (N = 3932). These data were paired to geographic coordinates of all adult level I and II trauma centers within an 8.0-km buffer of each city. Between February and September 2018, small-area analyses were conducted to assess trauma desert status as a function of neighborhood racial/ethnic composition, and geospatial analyses were conducted to examine statistically significant trauma desert hot spots.
Main outcomes and measures: In small-area analyses, a trauma desert was defined as travel distance greater than 8.0 km to the nearest adult level I or level II trauma center. In geospatial analyses, relative trauma deserts were identified using travel distance as a continuous measure. Census tracts were classified into (1) racial/ethnic composition categories, based on patterns of residential segregation, including white majority, black majority, Hispanic/Latino majority, and other or integrated; and (2) poverty categories, including nonpoor and poor.
Results: Chicago, LA, and NYC contained 798, 1006, and 2128 census tracts, respectively. A large proportion comprised a black majority population in Chicago (35.1%) and NYC (21.4%), compared with LA (2.7%). In primary analyses, black majority census tracts were more likely than white majority census tracts to be located in a trauma desert in Chicago (odds ratio [OR], 8.48; 95% CI, 5.71-12.59) and LA (OR, 5.11; 95% CI, 1.50-17.39). In NYC, racial/ethnic disparities were not significant in unadjusted models, but were significant in models adjusting for poverty and race-poverty interaction effects (adjusted OR, 1.87; 95% CI, 1.27-2.74). In comparison, Hispanic/Latino majority census tracts were less likely to be located in a trauma desert in NYC (OR, 0.03; 95% CI, 0.01-0.11) and LA (OR, 0.30; 95% CI, 0.22-0.40), but slightly more likely in Chicago (OR, 2.38; 95% CI, 1.56-3.64).
Conclusions and relevance: In this study, black majority census tracts were the only racial/ethnic group that appeared to be associated with disparities in geographic access to trauma centers.
Conflict of interest statement
Figures
Comment in
-
Racial and Ethnic Disparities in Geographic Access to Trauma Care-A Multiple-Methods Study of US Urban Trauma Deserts.JAMA Netw Open. 2019 Mar 1;2(3):e190277. doi: 10.1001/jamanetworkopen.2019.0277. JAMA Netw Open. 2019. PMID: 30848802 No abstract available.
References
-
- Friedersdorf C. American carnage. The Atlantic https://www.theatlantic.com/politics/archive/2018/02/trump-carnage/553424/. Published February 15, 2018. Accessed April 19, 2018.
-
- Federal Bureau of Investigation Criminal Justice Information Services Division Uniform Crime Reporting (UCR) program: 2014; https://ucr.fbi.gov. Accessed April 19, 2018.
-
- Taylor R. Travel Time Reliability. Washington, DC: US Department of Transportation; 2017.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
