

Topography of Simulated Intestinal Equilibrium Solubility
- PMID: 30848917
- PMCID: PMC6505523
- DOI: 10.1021/acs.molpharmaceut.8b01238
Topography of Simulated Intestinal Equilibrium Solubility
Abstract
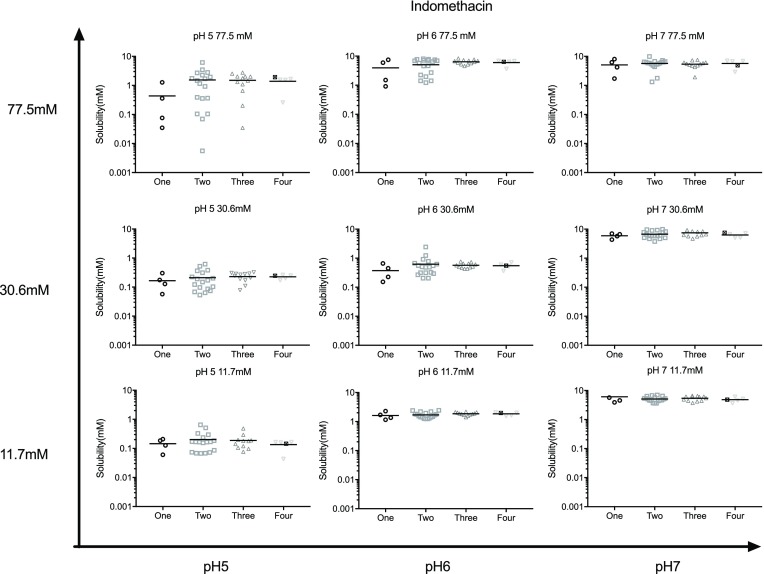
Oral administration of a solid dosage form requires drug dissolution in the gastrointestinal tract before absorption. Solubility is a key factor controlling dissolution, and it is recognized that, within the intestinal tract, this is influenced by the luminal fluid pH, amphiphile content, and composition. Various simulated intestinal fluid recipes have been introduced to mimic this behavior and studied using a range of different experimental techniques. In this article, we have measured equilibrium solubility utilizing a novel four component mixture design (4CMD) with biorelevant amphiphiles (bile salt, phospholipid, oleate, and monoglyceride) within a matrix of three pH values (5, 6, and 7) and total amphiphile concentrations (11.7, 30.6, and 77.5 mM) to provide a topographical and statistical overview. Three poorly soluble drugs representing acidic (indomethacin), basic (carvedilol), and neutral (fenofibrate) categories have been studied. The macroscopic solubility behavior agrees with literature and exhibits an overall increasing solubility from low pH and total amphiphile concentration to high pH and total amphiphile concentration. Within the matrix, all three drugs display different topographies, which can be related to the statistical effect levels of the individual amphiphiles or amphiphile interactions on solubility. The study also identifies previously unreported three and four way factor interactions notably between bile salt, phospholipid, pH, and total amphiphile concentration. In addition, the results also reveal that solubility variability is linked to the number of amphiphiles and the respective ratios in the measurement fluid, with the minimum variation present in systems containing all four amphiphiles. The individual 4CMD experiments within the matrix can be linked to provide a possible intestinal solubility window for each drug that could be applied in PBPK modeling systems. Overall the approach provides a novel overview of intestinal solubility topography along with greater detail on the impact of the various factors studied; however, each matrix requires 351 individual solubility measurements. Further studies will be required to refine the experimental protocol in order the maximize information garnered while minimizing the number of measurements required.
Keywords: Biopharmaceutics Classification System; FaSSIF; FeSSIF; IVIVC; four component mixture design; pH; solubility; total amphiphile concentration.
Conflict of interest statement
The authors declare no competing financial interest.
Figures







References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
