

Efficacy and safety of primary posterior capsulotomy in combined phaco-vitrectomy in rhegmatogenous retinal detachment
- PMID: 30849095
- PMCID: PMC6407776
- DOI: 10.1371/journal.pone.0213457
Efficacy and safety of primary posterior capsulotomy in combined phaco-vitrectomy in rhegmatogenous retinal detachment
Abstract
Objective: To evaluate the efficacy and safety of posterior capsulotomy by analyzing the long-term visual outcomes in patients with rhegmatogenous retinal detachment (RD), who underwent combined phaco-vitrectomy with or without primary posterior capsulotomy.
Methods: A retrospective longitudinal cohort analysis was performed by using data of rhegmatogenous RD patients undergoing combined phaco-vitrectomy. Patients were divided into two groups; Group A (68 eyes of 68 patients) with capsulotomy, and Group B (39 eyes of 39 patients) without capsulotomy. We reviewed the best-corrected visual acuity (BCVA), incidence of posterior capsule opacification (PCO), clinical features at the diagnosis of rhegmatogenous RD, and intraoperative or postoperative complications following posterior capsulotomy.
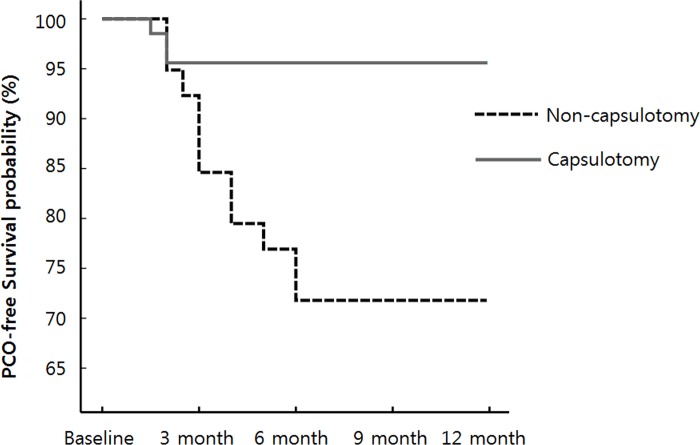
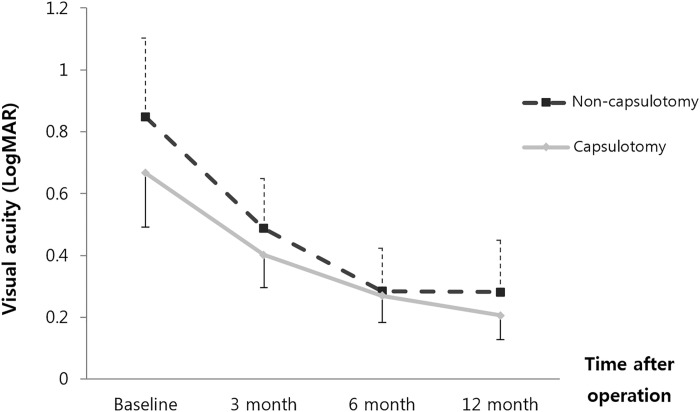
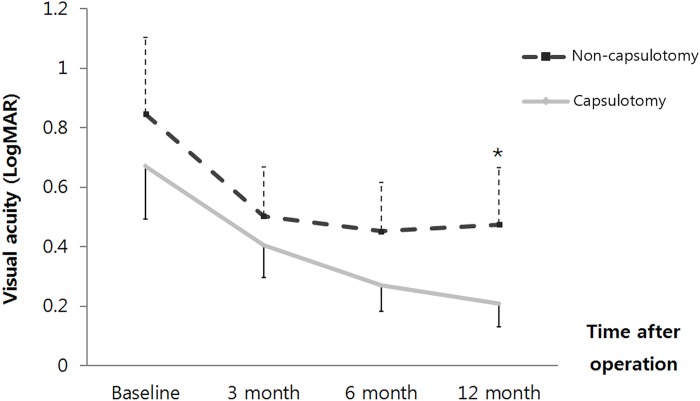
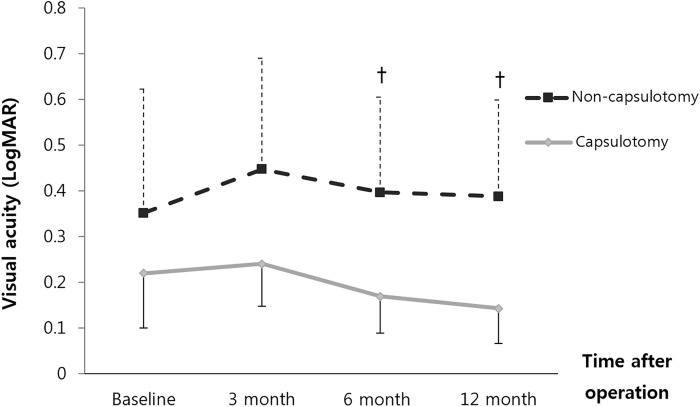
Results: The modified BCVA measured by the logarithm of the minimum angle of resolution at initial diagnosis and 3, 6, and 12 months after surgery was 0.67 in Group A versus 0.85 in Group B (p = 0.258), 0.40 in Group A versus 0.50 in Group B (p = 0.309), 0.27 in Group A versus 0.45 in Group B (p = 0.055), and 0.21 in Group A versus 0.47 in Group B (p = 0.014), respectively. In subgroup with macula-on RRD, Group A exhibited better visual outcomes compared to Group B at 6(0.17 versus 0.40 [p = 0.037]) and at 12 months(0.14 versus 0.39 [p = 0.030]). The incidence of PCO in Group B was higher than Group A(28.2% versus 4.4% (p < 0.001)). There were no complications associated with posterior capsulotomy.
Conclusions: A primary posterior capsulotomy during combined phaco-vitrectomy using a 23-gauge vitreous cutter was a safe and effective surgical procedure in patients with RRD patients for preventing postoperative intraocular lens-related PCO.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
Outcomes of 23-gauge pars plana vitrectomy combined with phacoemulsification and capsulotomy without intraocular lens implantation in rhegmatogenous retinal detachment associated with choroidal detachment.Medicine (Baltimore). 2017 Aug;96(34):e7869. doi: 10.1097/MD.0000000000007869. Medicine (Baltimore). 2017. PMID: 28834901 Free PMC article.
-
Influence of the "Inverted U Method" Nd: YAG Laser Posterior Capsulotomy on Anterior Segment Parameters, Decentration and Tilt of Intraocular Lens in Patients after Phaco-vitrectomy.Semin Ophthalmol. 2021 Apr 3;36(3):88-93. doi: 10.1080/08820538.2021.1884267. Epub 2021 Mar 18. Semin Ophthalmol. 2021. PMID: 33734918
-
Efficacy of combined 25-gauge microincision vitrectomy, intraocular lens implantation, and posterior capsulotomy.J Cataract Refract Surg. 2012 Sep;38(9):1602-7. doi: 10.1016/j.jcrs.2012.05.028. J Cataract Refract Surg. 2012. PMID: 22906446
-
Internal limiting membrane peeling versus no peeling during primary vitrectomy for rhegmatogenous retinal detachment: A systematic review and meta-analysis.PLoS One. 2018 Jul 19;13(7):e0201010. doi: 10.1371/journal.pone.0201010. eCollection 2018. PLoS One. 2018. PMID: 30024983 Free PMC article.
-
Combined versus Sequential Phacoemulsification and Pars Plana Vitrectomy: A Meta-Analysis.Ophthalmol Retina. 2021 Nov;5(11):1125-1138. doi: 10.1016/j.oret.2021.01.004. Epub 2021 Jan 20. Ophthalmol Retina. 2021. PMID: 33482399
Cited by
-
Comparison of simultaneous vs sequential pars plana vitrectomy and cataract surgery.BMC Ophthalmol. 2023 Feb 23;23(1):74. doi: 10.1186/s12886-023-02801-y. BMC Ophthalmol. 2023. PMID: 36823593 Free PMC article.
-
Efficacy and safety of primary posterior capsulotomy during phaco-vitrectomy for epiretinal membrane.BMC Ophthalmol. 2022 Jan 3;22(1):4. doi: 10.1186/s12886-021-02226-5. BMC Ophthalmol. 2022. PMID: 34980021 Free PMC article.
-
Novel Technique of Pneumatic Posterior Capsulorhexis for Treatment and Prevention of Posterior Capsular Opacification.J Ophthalmol. 2019 Dec 21;2019:3174709. doi: 10.1155/2019/3174709. eCollection 2019. J Ophthalmol. 2019. PMID: 31949950 Free PMC article.
References
-
- McDonnell PJ, Zarbin MA, Green WR. Posterior capsule opacification in pseudophakic eyes. Ophthalmology. 1983;90(12):1548–53. Epub 1983/12/01. . - PubMed
-
- Kappelhof JP, Vrensen GF. The pathology of after-cataract. A minireview. Acta ophthalmologica Supplement. 1992;(205):13–24. Epub 1992/01/01. . - PubMed
-
- Kumagai K, Ogino N, Shinjo U, Demizu S, Shioya M, Ueda K. Vitreous opacification after neodymium:YAG posterior capsulotomy. Journal of cataract and refractive surgery. 1999;25(7):981–4. Epub 1999/07/15. . - PubMed
-
- Slomovic AR, Parrish RK, 2nd. Acute elevations of intraocular pressure following Nd:YAG laser posterior capsulotomy. Ophthalmology. 1985;92(7):973–6. Epub 1985/07/01. . - PubMed
-
- Steinert RF, Puliafito CA, Kumar SR, Dudak SD, Patel S. Cystoid macular edema, retinal detachment, and glaucoma after Nd:YAG laser posterior capsulotomy. American journal of ophthalmology. 1991;112(4):373–80. Epub 1991/10/15. . - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
