

Inequitable coverage of vitamin A supplementation in Nigeria and implications for childhood blindness
- PMID: 30849959
- PMCID: PMC6408825
- DOI: 10.1186/s12889-019-6413-1
Inequitable coverage of vitamin A supplementation in Nigeria and implications for childhood blindness
Abstract
Background: Vitamin A deficiency (VAD) is of major public health significance; it is a risk factor for childhood deaths from diarrhoea and measles in low and middle-income countries and an important cause of preventable childhood blindness in low income countries. Vitamin A supplementation (VAS) is being implemented in many LMICs and high coverage reduces the prevalence of blinding corneal diseases in children. However, national estimates of coverage may not reveal any inequities in intra country coverage. The aim of this study is to assess factors influencing VAS coverage and also assess the relationship between VAS coverage and childhood corneal blindness in Nigeria.
Methods: Data were collected from the Nigeria Demographic and Health Survey (NDHS) 2013 and the published literature on population-based childhood blindness surveys in Nigeria. The main outcome measure was the proportion of eligible children who received VAS in the last 6 months preceding the survey. Study factors comprised a range of socioeconomic, and individual factors. Data were analysed using STATA V.12.1 (Statcorp, Texas). To explore the effects of the independent variables on VAS coverage, bivariate and multivariate regression was done. Variables with p < 0.05 in the final multivariable model were considered as independent factors. For the population-based childhood blindness surveys, aggregated and disaggregated data were used. Causes of blindness were stratified into corneal blindness and 'others'. Odds ratios were computed to determine the odds of developing corneal blindness in each geopolitical region. Tests of significance were set at the 95% level.
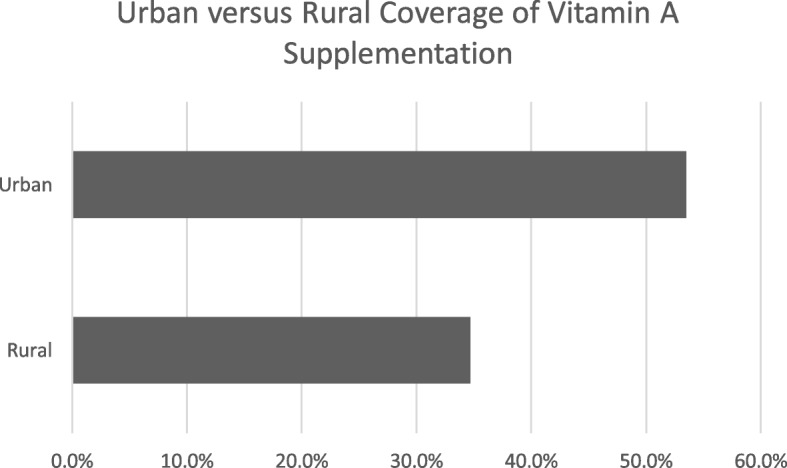
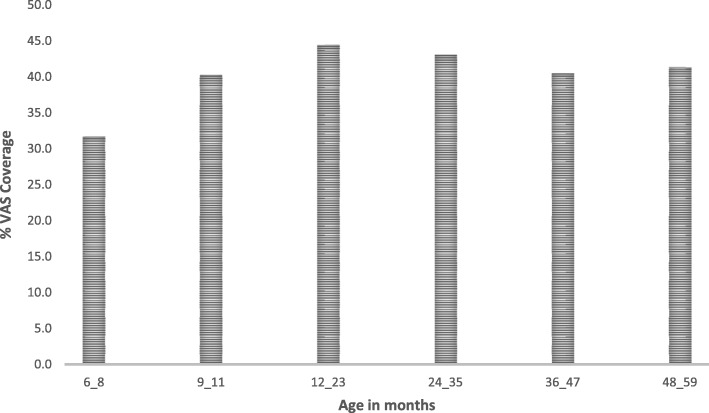
Results: The total VAS coverage in 2013 was 41.5%. VAS coverage was inequitable. Children with very educated mothers (OR 3.27 p < 0.001), from the south-south region (OR 2.38 p < 0.001) or in the highest wealth quintile (OR 2.81 p < 0.001) had higher odds of receiving VAS. The northwest zone had the lowest VAS coverage and the highest prevalence of corneal blindness.
Conclusion: Regional and socioeconomic inequities in VAS exist in Nigeria and these may have grave implications for the causes of childhood blindness. The development and implementation of context specific and effective strategies are needed to reduce these inequities in VAS.
Keywords: Childhood blindness; Nigeria; Vitamin A supplementation.
Conflict of interest statement
Ethics approval and consent to participate
Ethical clearance for the NDHS 2013 was obtained from the National Health Research Ethic Committee (NHREC) in Nigeria, before the survey was conducted [16]. In addition, permission to use the data was obtained from MEASURE DHS/ICF Macro International, the agency responsible for the worldwide Demographic and Health Surveys.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Stevens GA, Bennett JE, Hennocq Q, Lu Y, De-Regil LM, Rogers L, et al. Trends and mortality effects of vitamin A deficiency in children in 138 low-income and middle-income countries between 1991 and 2013: a pooled analysis of population-based surveys. Lancet Glob Health. 2015;3(9):e528–ee36. doi: 10.1016/S2214-109X(15)00039-X. - DOI - PubMed
-
- World Health Organization . Global prevalence of vitamin A deficiency in populations at risk 1995-2005: WHO global database on vitamin A deficiency. 2009.
-
- UNICEF Division of Communication . In: Tracking progress on child and maternal nutrition: a survival and development priority. UNICEF, editor. 2009.
-
- Dalmiya N, Palmer A. Vitamin A supplementation: a decade of progress: UNICEF. 2007.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
