

Chlorhexidine versus routine bathing to prevent multidrug-resistant organisms and all-cause bloodstream infections in general medical and surgical units (ABATE Infection trial): a cluster-randomised trial
- PMID: 30850112
- PMCID: PMC6650266
- DOI: 10.1016/S0140-6736(18)32593-5
Chlorhexidine versus routine bathing to prevent multidrug-resistant organisms and all-cause bloodstream infections in general medical and surgical units (ABATE Infection trial): a cluster-randomised trial
Erratum in
-
Department of Error.Lancet. 2019 Mar 23;393(10177):1204. doi: 10.1016/S0140-6736(19)30647-6. Lancet. 2019. PMID: 30910304 No abstract available.
-
Department of Error.Lancet. 2019 Aug 10;394(10197):470. doi: 10.1016/S0140-6736(19)31768-4. Epub 2019 Aug 8. Lancet. 2019. PMID: 31402028 No abstract available.
Abstract
Background: Universal skin and nasal decolonisation reduces multidrug-resistant pathogens and bloodstream infections in intensive care units. The effect of universal decolonisation on pathogens and infections in non-critical-care units is unknown. The aim of the ABATE Infection trial was to evaluate the use of chlorhexidine bathing in non-critical-care units, with an intervention similar to one that was found to reduce multidrug-resistant organisms and bacteraemia in intensive care units.
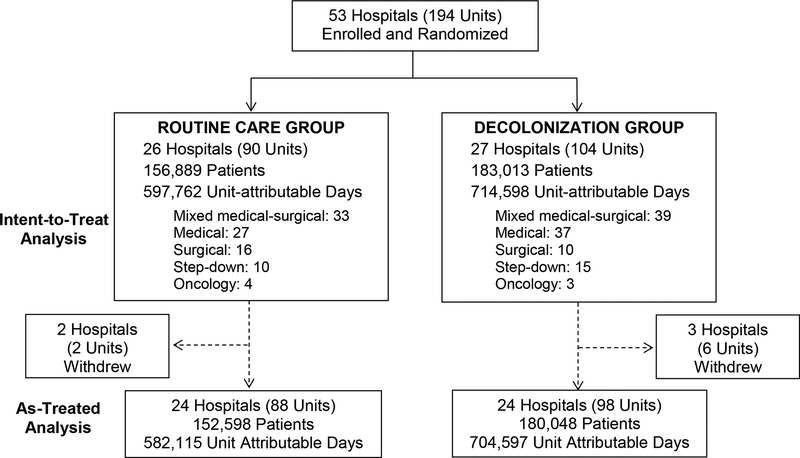
Methods: The ABATE Infection (active bathing to eliminate infection) trial was a cluster-randomised trial of 53 hospitals comparing routine bathing to decolonisation with universal chlorhexidine and targeted nasal mupirocin in non-critical-care units. The trial was done in hospitals affiliated with HCA Healthcare and consisted of a 12-month baseline period from March 1, 2013, to Feb 28, 2014, a 2-month phase-in period from April 1, 2014, to May 31, 2014, and a 21-month intervention period from June 1, 2014, to Feb 29, 2016. Hospitals were randomised and their participating non-critical-care units assigned to either routine care or daily chlorhexidine bathing for all patients plus mupirocin for known methicillin-resistant Staphylococcus aureus (MRSA) carriers. The primary outcome was MRSA or vancomycin-resistant enterococcus clinical cultures attributed to participating units, measured in the unadjusted, intention-to-treat population as the HR for the intervention period versus the baseline period in the decolonisation group versus the HR in the routine care group. Proportional hazards models assessed differences in outcome reductions across groups, accounting for clustering within hospitals. This trial is registered with ClinicalTrials.gov, number NCT02063867.
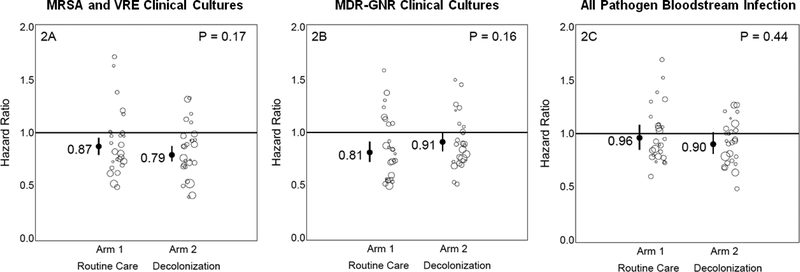
Findings: There were 189 081 patients in the baseline period and 339 902 patients (156 889 patients in the routine care group and 183 013 patients in the decolonisation group) in the intervention period across 194 non-critical-care units in 53 hospitals. For the primary outcome of unit-attributable MRSA-positive or VRE-positive clinical cultures (figure 2), the HR for the intervention period versus the baseline period was 0·79 (0·73-0·87) in the decolonisation group versus 0·87 (95% CI 0·79-0·95) in the routine care group. No difference was seen in the relative HRs (p=0·17). There were 25 (<1%) adverse events, all involving chlorhexidine, among 183 013 patients in units assigned to chlorhexidine, and none were reported for mupirocin.
Interpretation: Decolonisation with universal chlorhexidine bathing and targeted mupirocin for MRSA carriers did not significantly reduce multidrug-resistant organisms in non-critical-care patients.
Funding: National Institutes of Health.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of Interests
Sage Products and Molnlycke contributed antiseptic Chlorhexidine product to this trial. Investigators are also conducting other studies in which contributed antiseptic product is provided to participating hospitals and nursing homes from Stryker (Sage Products) (KK, LH, MHC, MKH, RAW, SSH), 3M (LH, SSH), Clorox (CS, ES, JH, JM, JP, KH, KK, LH, LS, MHC, MKH, RAW, RP, SSH, TRA), Xttrium (LH, SSH), and Medline (CS, ES, JH, JM, JP, KH, KK, LH, LS, MHC, MKH, RAW, RP, SSH, TRA). Investigator-initiated grant funds were received from Clorox (MKH, MHC, LS, KH, RP). Companies contributing product or providing grant funds have no role in the design, conduct, analysis, or publication of the ABATE Infection Trial or other studies conducted by these investigators. All other authors have no disclosures.
Figures
Comment in
-
No benefit of chlorhexidine bathing in non-critical care units.Lancet. 2019 Mar 23;393(10177):1179-1180. doi: 10.1016/S0140-6736(18)33130-1. Epub 2019 Mar 5. Lancet. 2019. PMID: 30850113 No abstract available.
References
-
- National and state healthcare associated infections. Centers for Disease Control and Prevention. 2016. https://www.cdc.qov/HAI/pdfs/proqress-report/hai-proqress-report.pdf
-
- Maki DG, Ringer M, Alvarado CJ. Prospective randomised trial of povidone-iodine, alcohol, and Chlorhexidine for prevention of infection associated with central venous and arterial catheters. Lancet. 1991. August 10;338(8763):339–43. - PubMed
-
- Mimoz O, Lucet JC, Kerforne T et al. Skin antisepsis with chlorhexidine-alcohol versus povidone iodine-alcohol, with and without skin scrubbing, for prevention of intravascular-catheter-related infection (CLEAN): an open-label, multicentre, randomised, controlled, two-by-two factorial trial. Lancet. 2015;386(10008):2069–2077. - PubMed
-
- Raad I, Darouiche R, Dupuis J, et al. Central venous catheters coated with minocycline and rifampin for the prevention of catheter-related colonization and bloodstream infections. A randomized, double-blind trial. The Texas Medical Center Catheter Study Group. Ann Intern Med. 1997. August 15;127(4):267–74. - PubMed
-
- de Smet AM, Kluytmans JA, Cooper BS, et al. Decontamination of the digestive tract and oropharynx in ICU patients. N Engl J Med. 2009. January 1;360(1):20–31. - PubMed
