

Mas receptor deficiency augments angiotensin II-induced atherosclerosis and aortic aneurysm ruptures in hypercholesterolemic male mice
- PMID: 30850299
- PMCID: PMC6728232
- DOI: 10.1016/j.jvs.2018.11.045
Mas receptor deficiency augments angiotensin II-induced atherosclerosis and aortic aneurysm ruptures in hypercholesterolemic male mice
Abstract
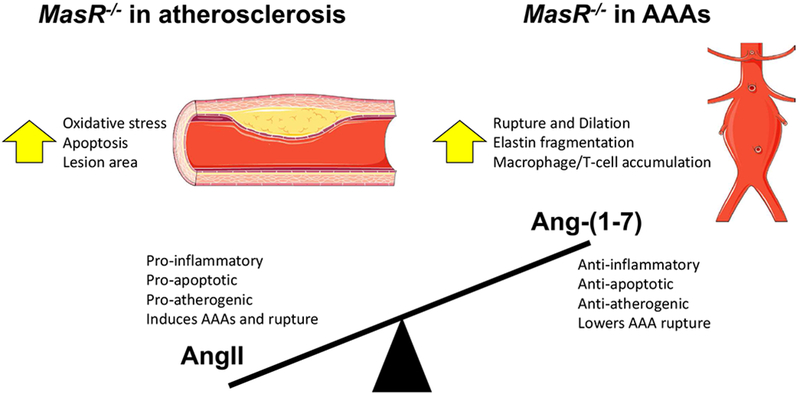
Objective: Previous studies demonstrated that deficiency of angiotensin-converting enzyme 2 (ACE2) augmented angiotensin II (AngII)-induced atherosclerosis and abdominal aortic aneurysm (AAA) formation in hypercholesterolemic mice. Effects of ACE2 deficiency could arise from increased concentrations of its substrate, AngII, or decreased concentrations of its product, angiotensin-(1-7) [Ang-(1-7)]. Infusion of Ang-(1-7), a Mas receptor (MasR) ligand, to hypercholesterolemic male mice reduced AngII-induced atherosclerosis, suggesting a protective role of the Ang-(1-7)/MasR axis. However, it is unclear whether endogenous Ang-(1-7) acts at MasR to influence AngII-induced vascular diseases. The purpose of this study was to define the role of MasR deficiency in AngII-induced atherosclerosis and AAA formation and severity in hypercholesterolemic male mice.
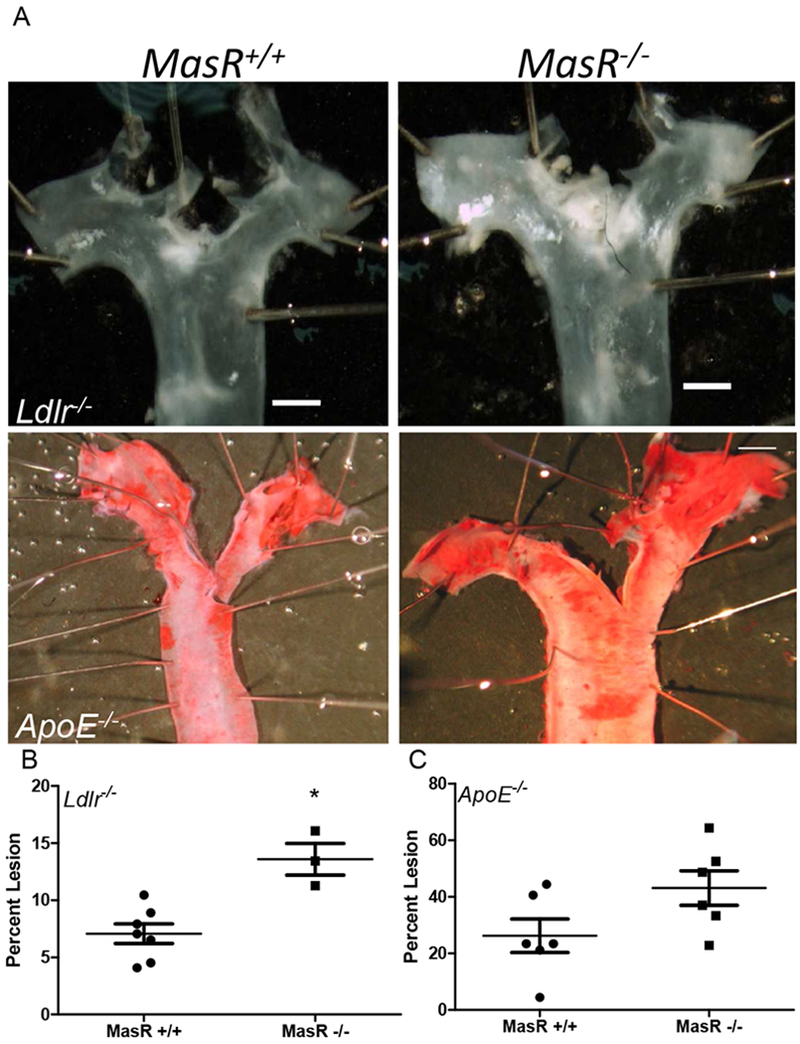
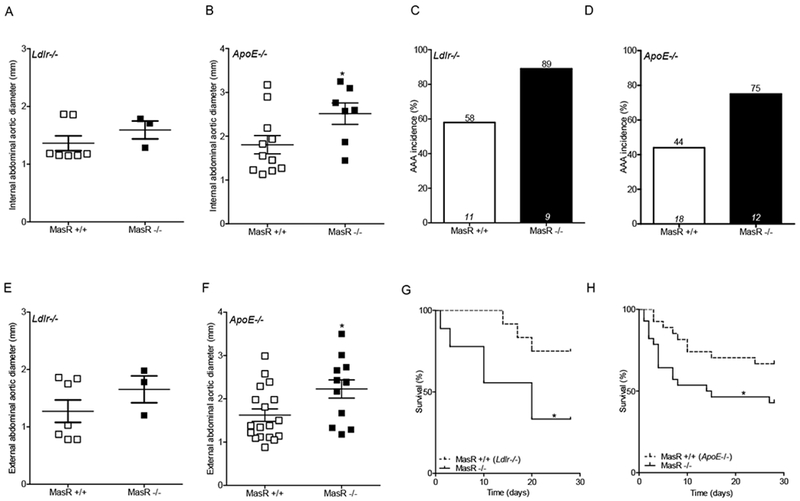
Methods: MasR+/+ and MasR-/- male mice on a low-density lipoprotein receptor-deficient (Ldlr-/-) or apolipoprotein E-deficient (Apoe-/-) background were infused with AngII at either 600 or 1000 ng/kg/min by osmotic minipump for 28 days. Atherosclerosis was quantified at study end point as percentage lesion surface area of the aortic arch in Ldlr-/- mice. Abdominal aortic internal diameters were quantified by ultrasound, and maximal external AAA diameters were quantified at study end point. Blood pressure was quantified by radiotelemetry and a tail cuff-based technique. Serum cholesterol concentrations and vascular tissue characterization were examined at study end point.
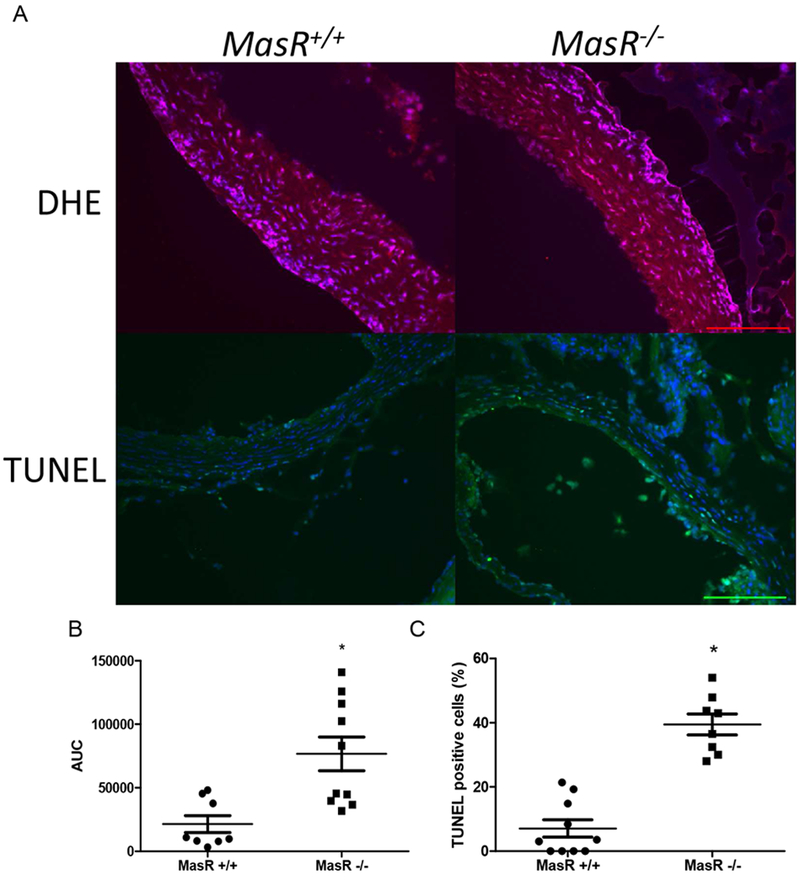
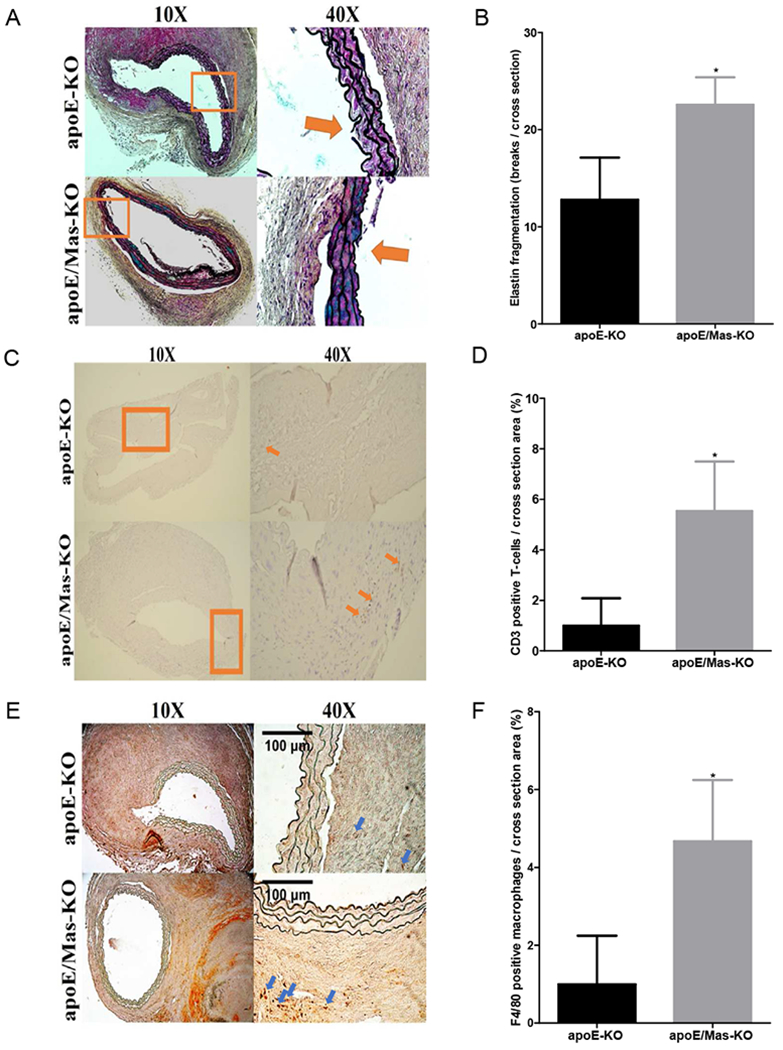
Results: MasR deficiency did not influence body weight, systolic blood pressure at baseline and during AngII infusion, or serum cholesterol concentrations in either Apoe-/- or Ldlr-/- mice. MasR deficiency increased AngII-induced atherosclerosis in aortic arches of Ldlr-/- mice (P < .05), associated with increased oxidative stress and apoptosis in aortic root sections (P < .05). MasR deficiency also augmented internal and external AAA diameters and increased aortic ruptures of both Ldlr-/- and Apoe-/- mice (P < .05). These effects were associated with increased elastin breaks and T-lymphocyte and macrophage accumulation into abdominal aortas of AngII-infused MasR-deficient mice (P < .05).
Conclusions: These results demonstrate that MasR deficiency augmented AngII-induced atherosclerosis and AAA rupture through mechanisms involving increased oxidative stress, inflammation, and apoptosis, suggesting that MasR activation may provide therapeutic efficacy against vascular diseases.
Keywords: Aneurysm; Angiotensin-(1-7); Atherosclerosis; Mas receptor; Rupture.
Copyright © 2019 Society for Vascular Surgery. All rights reserved.
Figures
Comment in
-
Invited commentary.J Vasc Surg. 2019 Nov;70(5):1668. doi: 10.1016/j.jvs.2019.01.031. J Vasc Surg. 2019. PMID: 31653380 No abstract available.
References
-
- Cassis LA, Rateri DL, Lu H, Daugherty A. Bone marrow transplantation reveals that recipient AT1a receptors are required to initiate angiotensin II-induced atherosclerosis and aneurysms. Arteriosclerosis, thrombosis, and vascular biology. 2007;27(2):380–6. - PubMed
-
- Hayek T, Attias J, Smith J, Breslow JL, Keidar S. Antiatherosclerotic and antioxidative effects of captopril in apolipoprotein E-deficient mice. J Cardiovasc Pharmacol. 1998;31(4):540–4. - PubMed
-
- Investigators O, Yusuf S, Teo KK, Pogue J, Dyal L, Copland I, et al. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med. 2008;358(15):1547–59. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
