

Relative cerebral hyperperfusion during cardiopulmonary bypass is associated with risk for postoperative delirium: a cross-sectional cohort study
- PMID: 30851736
- PMCID: PMC6408763
- DOI: 10.1186/s12871-019-0705-y
Relative cerebral hyperperfusion during cardiopulmonary bypass is associated with risk for postoperative delirium: a cross-sectional cohort study
Abstract
Background: Our objective was to evaluate if changes in on-pump cerebral blood flow, relative to the pre-bypass baseline, are associated with the risk for postoperative delirium (POD) following cardiac surgery.
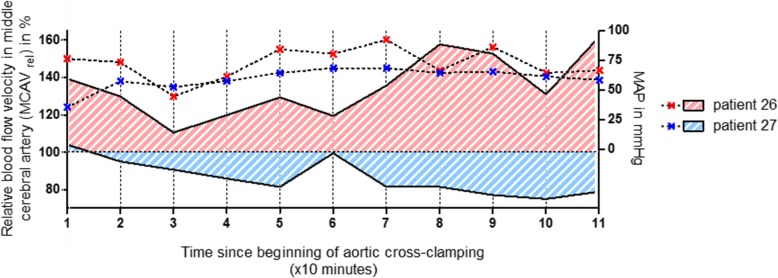
Methods: In 47 consecutive adult patients, right middle cerebral artery blood flow velocity (MCAV) was assessed using transcranial Doppler sonography. Individual values, measured during cardiopulmonary bypass (CPB), were normalized to the pre-bypass baseline value and termed MCAVrel. An MCAVrel > 100% was defined as cerebral hyperperfusion. Prevalence of POD was assessed using the Confusion Assessment Method for the Intensive Care Unit.
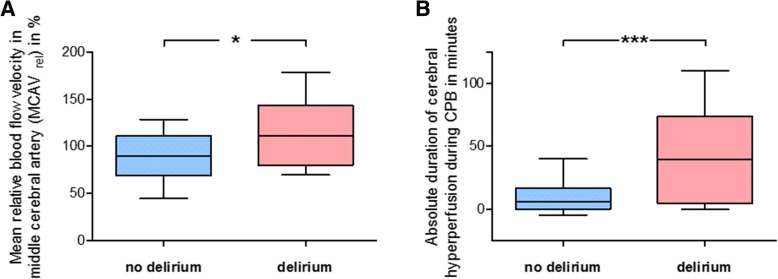
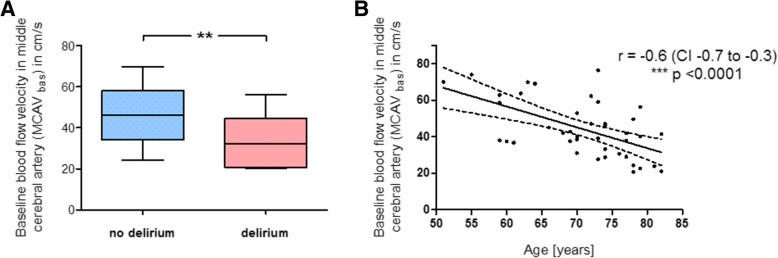
Results: Overall prevalence of POD was 27%. In the subgroup without POD, 32% of patients had experienced relative cerebral hyperperfusion during CPB, compared to 67% in the subgroup with POD (p < 0.05). The mean averaged MCAVrel was 90 (±21) % in the no-POD group vs. 112 (±32) % in the POD group (p < 0.05), and patients developing delirium experienced cerebral hyperperfusion during CPB for about 39 (±35) min, compared to 6 (±11) min in the group without POD (p < 0.001). In a subcohort with pre-bypass baseline MCAV (MCAVbas) below the median MCAVbas of the whole cohort, prevalence of POD was 17% when MCAVrel during CPB was kept below 100%, but increased to 53% when these patients actually experienced relative cerebral hyperperfusion.
Conclusions: Our results suggest a critical role for cerebral hyperperfusion in the pathogenesis of POD following on-pump open-heart surgery, recommending a more individualized hemodynamic management, especially in the population at risk.
Keywords: Cardiac surgery; Cardiopulmonary bypass; Cerebral blood flow; Delirium; Transcranial Doppler sonography.
Conflict of interest statement
Ethics approval and consent to participate
This observation was performed after approval by the institutional review board of the University of Bonn (protocol number 300/16, date of approval 2016-06-16). According to the approval, informed consent was waived.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
The association between cerebral blood flow variations during on-pump coronary artery bypass grafting surgery and postoperative delirium.Perfusion. 2025 Mar;40(2):440-449. doi: 10.1177/02676591241239823. Epub 2024 Mar 15. Perfusion. 2025. PMID: 38487837
-
The effect of relative cerebral hyperperfusion during cardiac surgery with cardiopulmonary bypass to delayed neurocognitive recovery.Perfusion. 2023 Nov;38(8):1688-1696. doi: 10.1177/02676591221129737. Epub 2022 Sep 23. Perfusion. 2023. PMID: 36148780 Free PMC article.
-
Cerebral Function and Perfusion during Cardiopulmonary Bypass: A Plea for a Multimodal Monitoring Approach.Heart Surg Forum. 2018 Jan 31;21(1):E028-E035. doi: 10.1532/hsf.1894. Heart Surg Forum. 2018. PMID: 29485961
-
Generation, detection and prevention of gaseous microemboli during cardiopulmonary bypass procedure.Int J Artif Organs. 2011 Nov;34(11):1039-51. doi: 10.5301/ijao.5000010. Int J Artif Organs. 2011. PMID: 22183517 Review.
-
Pre-operative biomarkers and imaging tests as predictors of post-operative delirium in non-cardiac surgical patients: a systematic review.BMC Anesthesiol. 2019 Feb 23;19(1):25. doi: 10.1186/s12871-019-0693-y. BMC Anesthesiol. 2019. PMID: 30797230 Free PMC article.
Cited by
-
Risk Factors for Delayed Neurocognitive Recovery According to Brain Biomarkers and Cerebral Blood Flow Velocity.Medicina (Kaunas). 2020 Jun 11;56(6):288. doi: 10.3390/medicina56060288. Medicina (Kaunas). 2020. PMID: 32545416 Free PMC article.
-
Extended neuromonitoring in aortic arch surgery : A case series.Anaesthesist. 2021 Dec;70(Suppl 1):68-73. doi: 10.1007/s00101-021-00983-y. Epub 2021 Jun 7. Anaesthesist. 2021. PMID: 34097082 Free PMC article.
-
[Near-infrared spectroscopy : Technique, development, current use and perspectives].Anaesthesist. 2021 Mar;70(3):190-203. doi: 10.1007/s00101-020-00837-z. Anaesthesist. 2021. PMID: 32930804 Review. German.
-
Cerebral Overperfusion Despite Reduced Cortical Metabolism Is Associated with Postoperative Delirium in Cardiac Surgery Patients: A Prospective Observational Study.J Clin Med. 2024 Nov 3;13(21):6605. doi: 10.3390/jcm13216605. J Clin Med. 2024. PMID: 39518743 Free PMC article.
-
Effect of cerebral oxygen saturation monitoring in patients undergoing superficial temporal anterior-middle cerebral artery anastomosis for ischemic Moyamoya disease: a prospective cohort study.Front Neurol. 2023 Sep 21;14:1226455. doi: 10.3389/fneur.2023.1226455. eCollection 2023. Front Neurol. 2023. PMID: 37808481 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
