

An Age-Based Framework for Evaluating Genome-Scale Sequencing Results in Newborn Screening
- PMID: 30851990
- PMCID: PMC6535354
- DOI: 10.1016/j.jpeds.2018.12.027
An Age-Based Framework for Evaluating Genome-Scale Sequencing Results in Newborn Screening
Abstract
Objective: To assess the performance of a standardized, age-based metric for scoring clinical actionability to evaluate conditions for inclusion in newborn screening and compare it with the results from other contemporary methods.
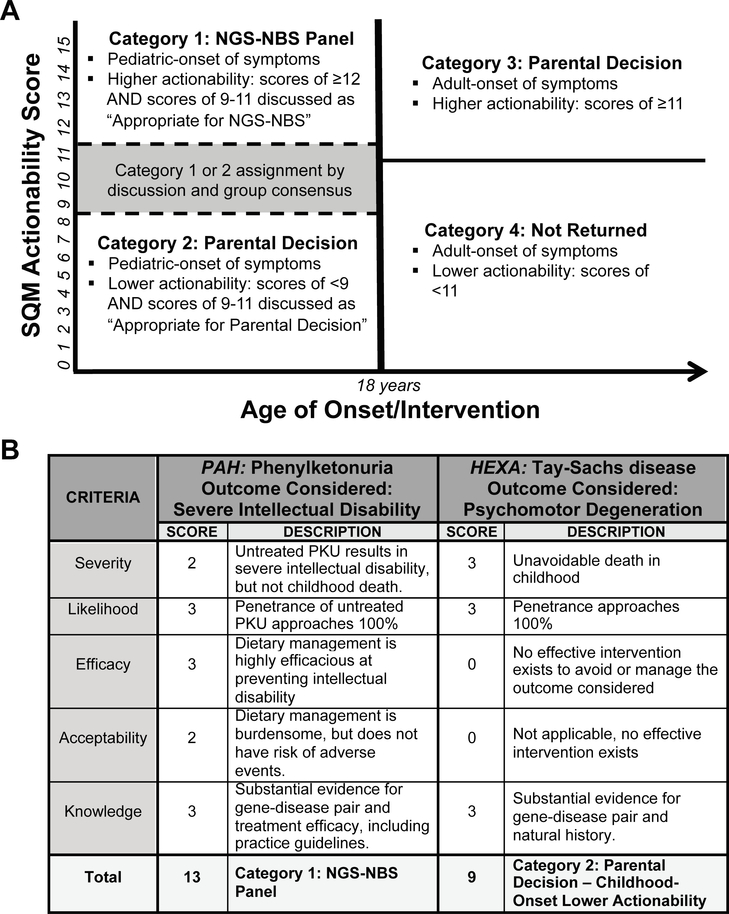
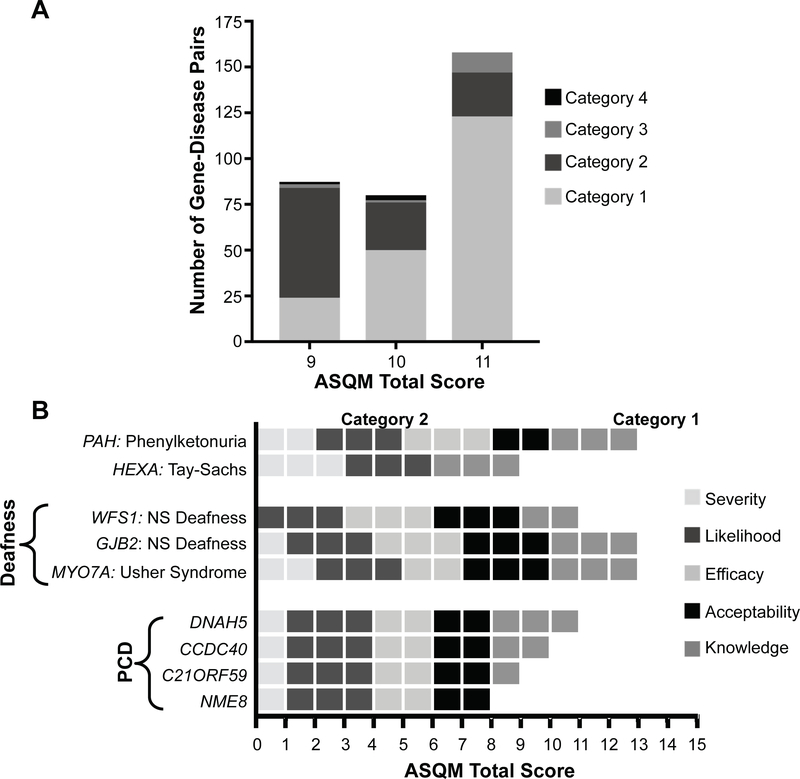
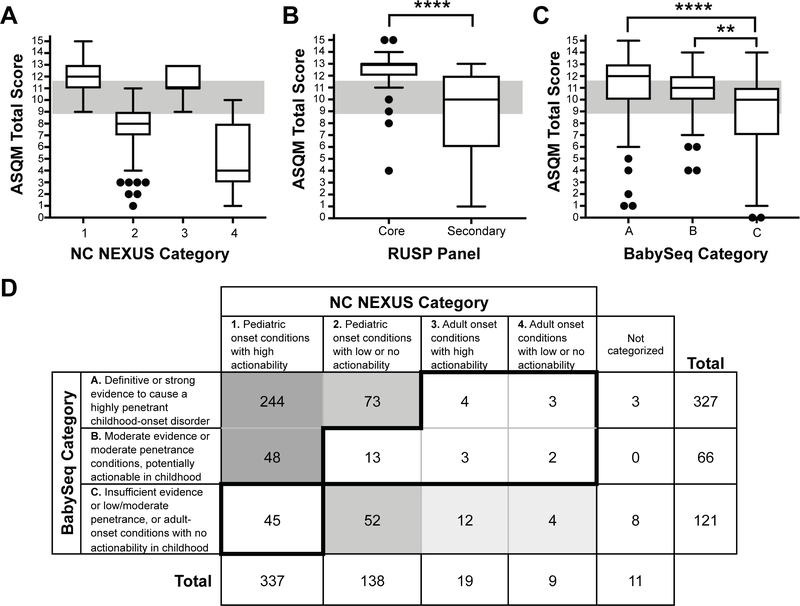
Study design: The North Carolina Newborn Exome Sequencing for Universal Screening study developed an age-based, semiquantitative metric to assess the clinical actionability of gene-disease pairs and classify them with respect to age of onset or timing of interventions. This categorization was compared with the gold standard Recommended Uniform Screening Panel and other methods to evaluate gene-disease pairs for newborn genomic sequencing.
Results: We assessed 822 gene-disease pairs, enriched for pediatric onset of disease and suspected actionability. Of these, 466 were classified as having childhood onset and high actionability, analogous to conditions selected for the Recommended Uniform Screening Panel core panel. Another 245 were classified as having childhood onset and low to no actionability, 25 were classified as having adult onset and high actionability, 19 were classified as having adult onset and low to no actionability, and 67 were excluded due to controversial evidence and/or prenatal onset.
Conclusions: This study describes a novel method to facilitate decisions about the potential use of genomic sequencing for newborn screening. These categories may assist parents and physicians in making informed decisions about the disclosure of results from voluntary genomic sequencing in children.
Keywords: ASQM; NC NEXUS; NGS-NBS; NSIGHT; actionability; decision-making; disclosure; genetics.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures
Comment in
-
Large Scale Next Generation Sequencing and Newborn Screening: Are We Ready?J Pediatr. 2019 Jun;209:9-10. doi: 10.1016/j.jpeds.2019.01.037. Epub 2019 Feb 25. J Pediatr. 2019. PMID: 30819502 No abstract available.
References
-
- Newborn screening: A blueprint for the future executive summary: newborn screening task force report. Pediatrics. 2000;106:386–388. - PubMed
-
- American College of Medical Genetics Newborn Screening Expert Group. Newborn screening: toward a uniform screening panel and system-executive summary. Pediatrics. 2006;117:S296–307. - PubMed
-
- Wilcken B, Wiley V, Hammond J, Carpenter K. Screening newborns for inborn errors of metabolism by tandem mass spectrometry. N Engl J Med. 2003;348:2304–2312. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
