

Characterising variation in composition and activation criteria of rapid response and cardiac arrest teams: a survey of Medicare participating hospitals in five American states
- PMID: 30852537
- PMCID: PMC6429839
- DOI: 10.1136/bmjopen-2018-024548
Characterising variation in composition and activation criteria of rapid response and cardiac arrest teams: a survey of Medicare participating hospitals in five American states
Abstract
Objectives: To characterise the variation in composition, leadership, and activation criteria of rapid response and cardiac arrest teams in five north-eastern states of the USA.
Design: Cross-sectional study consisting of a voluntary 46-question survey of acute care hospitals in north-eastern USA.
Setting: Acute care hospitals in New York, New Jersey, Rhode Island, Vermont, and Pennsylvania.
Participants: Surveys were completed by any member of the rapid response team (RRT) with a working knowledge of team composition and function. Participants were all Medicare-participating acute care hospitals, including teaching and community hospitals as well as hospitals from rural, urban and suburban areas.
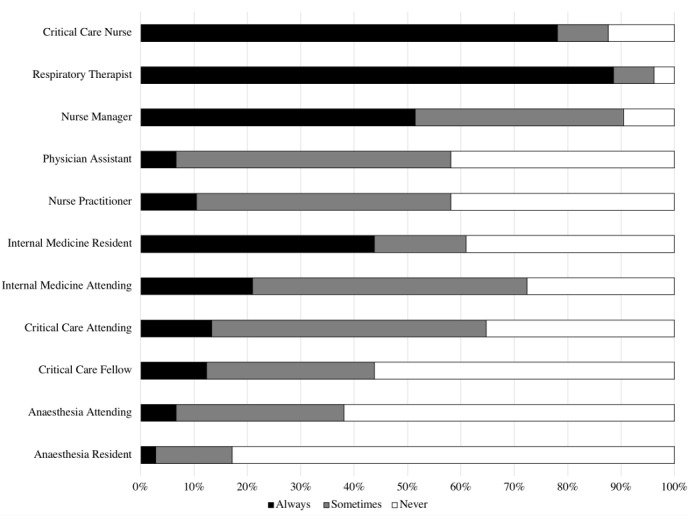
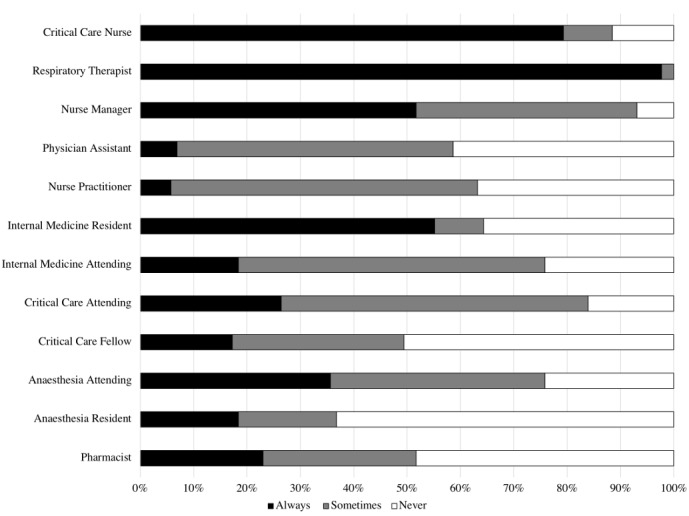
Results: Out of 378 hospitals, contacts were identified for 303, and 107 surveys were completed. All but two hospitals had an RRT, 70% of which changed members daily. The most common activation criteria were clinical concern (95%), single vital sign abnormalities (77%) and early warning score (59%). Eighty one per cent of hospitals had a dedicated cardiac arrest team.RRT composition varied widely, with respiratory therapists, critical care nurses, physicians and nurse managers being the most likely to attend (89%, 78%, 64% and 51%, respectively). Consistent presence of critical care physicians was uncommon and both cardiac arrest teams and teams were frequently led by trainee physicians, often without senior supervision.
Conclusions: As the largest study to date in the USA, we have demonstrated wide heterogeneity, rapid team turnover and a lack of senior supervision of RRT and cardiac arrest teams. These factors likely contribute to the mixed results seen in studies of RRTs.
Keywords: epidemiology.
© Author(s) (or their employer(s)) 2018. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Institute for Healthcare Improvement. 5 Million Lives campaign. 2006. http://www.ihi.org/about/documents/5millionlivescampaigncasestatement.pdf (accessed 10 Mar 2018).
-
- Bellomo R, Goldsmith D, Uchino S, et al. A prospective before-and-after trial of a medical emergency team. Med J Aust 2003;179:283–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials