

Social Factors, Sex, and Mortality Risk After Coronary Artery Bypass Grafting: A Population-Based Cohort Study
- PMID: 30852925
- PMCID: PMC6475039
- DOI: 10.1161/JAHA.118.011490
Social Factors, Sex, and Mortality Risk After Coronary Artery Bypass Grafting: A Population-Based Cohort Study
Abstract
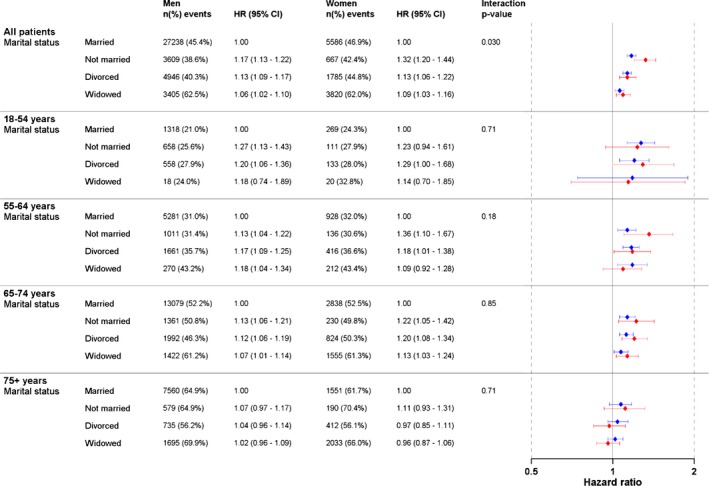
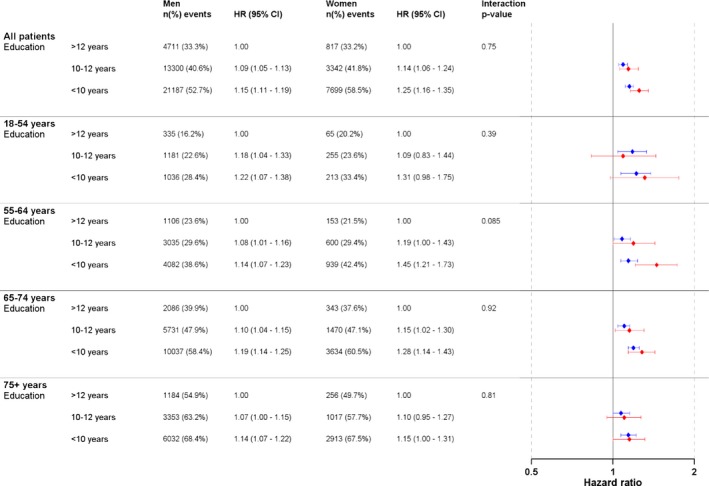
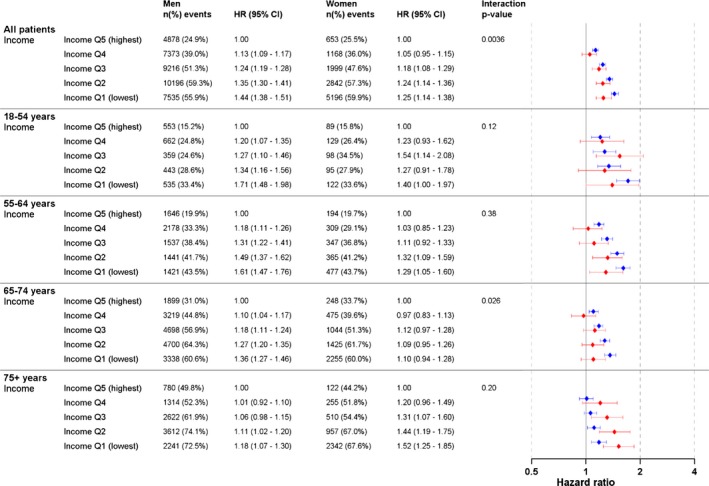
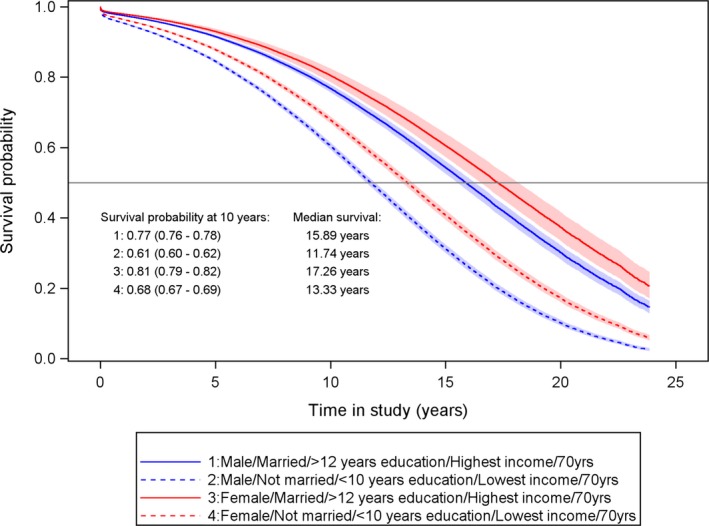
Background Little is known of the impact of social factors on mortality after coronary artery bypass grafting ( CABG ). We explored sex- and age-specific associations between mortality risk after CABG and marital status, income, and education. Methods and Results This population-based register study included 110 742 CABG patients (21.3% women) from the SWEDEHEART registry (Swedish Web-system for Enhancement and Development of Evidence-based Care in Heart Disease Evaluated According to Recommended Therapies) operated 1992 to 2015. Cox regression models were used to study the relation between social factors and all-cause mortality. Never having been married compared with being married/cohabiting was associated with a higher risk in women than in men (hazard ratio 1.32, 95% CI 1.20-1.44) versus 1.17 (1.13-1.22), P=0.030 between sex. The lowest income quintile, compared with the highest, was associated with higher risk in men than in women (hazard ratio 1.44 [1.38-1.51] versus 1.25 [1.14-1.38], P=0.0036). Lowest education level was associated with higher risk without sex difference (hazard ratio 1.15 [1.11-1.19] versus 1.25 [1.16-1.35], P=0.75). For unmarried women aged 60 years at surgery with low income and low education, mortality 10 years after surgery was 18%, compared with 11% in married women with high income and higher education level. The median life expectancy was 4.8 years shorter. Corresponding figures for 60-year-old men were 21% versus 12% mortality risk at 10 years and 5.0 years shorter life expectancy. Conclusions There are strong associations between social factors and mortality risk after CABG in both men and women. These results emphasize the importance of developing and implementing secondary prevention strategies for CABG patients with disadvantages in social factors.
Keywords: coronary artery bypass grafting; mortality; social inequalities; socioeconomic factors.
Figures

Similar articles
-
Socioeconomic Factors, Secondary Prevention Medication, and Long-Term Survival After Coronary Artery Bypass Grafting: A Population-Based Cohort Study From the SWEDEHEART Registry.J Am Heart Assoc. 2020 Mar 3;9(5):e015491. doi: 10.1161/JAHA.119.015491. Epub 2020 Mar 2. J Am Heart Assoc. 2020. PMID: 32114890 Free PMC article.
-
Does a similar procedure result in similar survival for women and men undergoing isolated coronary artery bypass grafting?J Thorac Cardiovasc Surg. 2017 Mar;153(3):571-579.e9. doi: 10.1016/j.jtcvs.2016.11.033. Epub 2016 Nov 21. J Thorac Cardiovasc Surg. 2017. PMID: 28108066
-
Coronary Artery Bypass Grafting in Women 50 Years or Younger.J Am Heart Assoc. 2019 Sep 17;8(18):e013211. doi: 10.1161/JAHA.119.013211. Epub 2019 Sep 14. J Am Heart Assoc. 2019. PMID: 31522591 Free PMC article.
-
Stroke Rates Following Surgical Versus Percutaneous Coronary Revascularization.J Am Coll Cardiol. 2018 Jul 24;72(4):386-398. doi: 10.1016/j.jacc.2018.04.071. J Am Coll Cardiol. 2018. PMID: 30025574
-
Effect of increasing age on percutaneous coronary intervention vs coronary artery bypass grafting in older adults with unprotected left main coronary artery disease: A meta-analysis and meta-regression.Clin Cardiol. 2019 Nov;42(11):1071-1078. doi: 10.1002/clc.23253. Epub 2019 Sep 5. Clin Cardiol. 2019. PMID: 31486094 Free PMC article. Review.
Cited by
-
Socioeconomic Factors and their Impact on Access and Use of Coronary and Structural Interventions.Eur Cardiol. 2022 Oct 27;17:e19. doi: 10.15420/ecr.2022.23. eCollection 2022 Feb. Eur Cardiol. 2022. PMID: 36643068 Free PMC article. Review.
-
Predictors of Premature Mortality Following Coronary Artery Bypass Grafting: An Iranian Single-Centre Study.Healthcare (Basel). 2023 Dec 23;12(1):36. doi: 10.3390/healthcare12010036. Healthcare (Basel). 2023. PMID: 38200942 Free PMC article.
-
Psychological Preparation for Cardiac Surgery.Curr Cardiol Rep. 2020 Oct 10;22(12):172. doi: 10.1007/s11886-020-01424-9. Curr Cardiol Rep. 2020. PMID: 33040263 Free PMC article. Review.
-
Socioeconomic factors and long-term mortality risk after surgical aortic valve replacement.Int J Cardiol Cardiovasc Risk Prev. 2023 Nov 8;19:200223. doi: 10.1016/j.ijcrp.2023.200223. eCollection 2023 Dec. Int J Cardiol Cardiovasc Risk Prev. 2023. PMID: 38023350 Free PMC article.
-
Experiences of informal caregivers after cardiac surgery: a systematic integrated review of qualitative and quantitative studies.BMJ Open. 2019 Nov 11;9(11):e032751. doi: 10.1136/bmjopen-2019-032751. BMJ Open. 2019. PMID: 31719093 Free PMC article.
References
-
- Havranek EP, Mujahid MS, Barr DA, Blair IV, Cohen MS, Cruz‐Flores S, Davey‐Smith G, Dennison‐Himmelfarb CR, Lauer MS, Lockwood DW, Rosal M, Yancy CW. Social determinants of risk and outcomes for cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2015;132:873–898. - PubMed
-
- Mackenbach JP, Cavelaars AE, Kunst AE, Groenhof F. Socioeconomic inequalities in cardiovascular disease mortality; an international study. Eur Heart J. 2000;21:1141–1151. - PubMed
-
- Rosengren A, Subramanian SV, Islam S, Chow CK, Avezum A, Kazmi K, Sliwa K, Zubaid M, Rangarajan S, Yusuf S. Education and risk for acute myocardial infarction in 52 high, middle and low‐income countries: INTERHEART case‐control study. Heart. 2009;95:2014–2022. - PubMed
-
- Bergstrom G, Redfors B, Angeras O, Dworeck C, Shao Y, Haraldsson I, Petursson P, Milicic D, Wedel H, Albertsson P, Ramunddal T, Rosengren A, Omerovic E. Low socioeconomic status of a patient's residential area is associated with worse prognosis after acute myocardial infarction in Sweden. Int J Cardiol. 2015;182:141–147. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
