

Evaluating Multisite rCBV Consistency from DSC-MRI Imaging Protocols and Postprocessing Software Across the NCI Quantitative Imaging Network Sites Using a Digital Reference Object (DRO)
- PMID: 30854448
- PMCID: PMC6403027
- DOI: 10.18383/j.tom.2018.00041
Evaluating Multisite rCBV Consistency from DSC-MRI Imaging Protocols and Postprocessing Software Across the NCI Quantitative Imaging Network Sites Using a Digital Reference Object (DRO)
Abstract
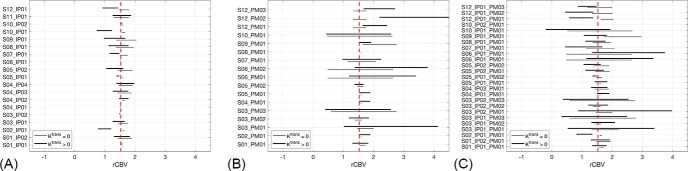
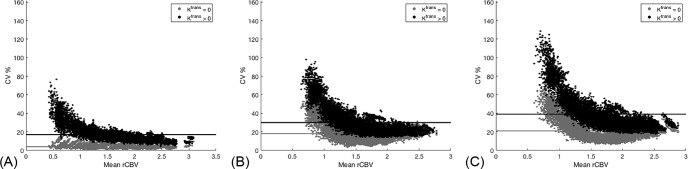
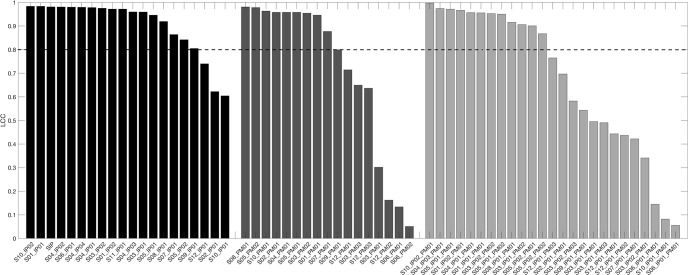
Relative cerebral blood volume (rCBV) cannot be used as a response metric in clinical trials, in part, because of variations in biomarker consistency and associated interpretation across sites, stemming from differences in image acquisition and postprocessing methods (PMs). This study leveraged a dynamic susceptibility contrast magnetic resonance imaging digital reference object to characterize rCBV consistency across 12 sites participating in the Quantitative Imaging Network (QIN), specifically focusing on differences in site-specific imaging protocols (IPs; n = 17), and PMs (n = 19) and differences due to site-specific IPs and PMs (n = 25). Thus, high agreement across sites occurs when 1 managing center processes rCBV despite slight variations in the IP. This result is most likely supported by current initiatives to standardize IPs. However, marked intersite disagreement was observed when site-specific software was applied for rCBV measurements. This study's results have important implications for comparing rCBV values across sites and trials, where variability in PMs could confound the comparison of therapeutic effectiveness and/or any attempts to establish thresholds for categorical response to therapy. To overcome these challenges and ensure the successful use of rCBV as a clinical trial biomarker, we recommend the establishment of qualifying and validating site- and trial-specific criteria for scanners and acquisition methods (eg, using a validated phantom) and the software tools used for dynamic susceptibility contrast magnetic resonance imaging analysis (eg, using a digital reference object where the ground truth is known).
Keywords: DSC-MRI; multisite consistency; relative cerebral blood volume; reproducibility; standardization.
Figures
References
-
- Boxerman JL, Ellingson BM, Jeyapalan S, Elinzano H, Harris RJ, Rogg JM, Pope WB, Safran H. Longitudinal DSC-MRI for distinguishing tumor recurrence from pseudoprogression in patients with a high-grade glioma. Am J Clin Oncol. 2014;0:1–7. - PubMed
-
- Ellingson BM, Zaw T, Cloughesy TF, Naeini KM, Lalezari S, Mong S, Lai A, Nghiemphu PL, Pope WB. Comparison between intensity normalization techniques for dynamic susceptibility contrast (DSC)-MRI estimates of cerebral blood volume (CBV) in human gliomas. J Magn Reson Imaging. 2012;35:1472–1477. - PubMed
-
- Chaskis C, Stadnik T, Michotte A, Van Rompaey K, D'Haens J. Prognostic value of perfusion-weighted imaging in brain glioma: a prospective study. Acta Neurochir (Wien). 2006;148:277–285. - PubMed
-
- Maia ACM, Malheiros SMF, da Rocha AJ, Stávale JN, Guimarães IF, Borges LR, Santos AJ, da Silva CJ, de Melo JG, Lanzoni OP, Gabbai AA, Ferraz FA. Stereotactic biopsy guidance in adults with supratentorial nonenhancing gliomas: role of perfusion-weighted magnetic resonance imaging. J Neurosurg. 2004;101:970–976. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
