

Nerve Compression Syndromes in the Posterior Cranial Fossa
- PMID: 30855007
- PMCID: PMC6415620
- DOI: 10.3238/arztebl.2019.0054
Nerve Compression Syndromes in the Posterior Cranial Fossa
Abstract
Background: Nerve compression syndromes in the posterior cranial fossa can severely impair patients' quality of life. There is often uncertainty about the best treatment. In this article, we provide an overview of these conditions and the corresponding treatment strategies.
Methods: This review is based on pertinent publications retrieved by a selective search in PubMed and on a scientific analysis of the authors' patient collective.
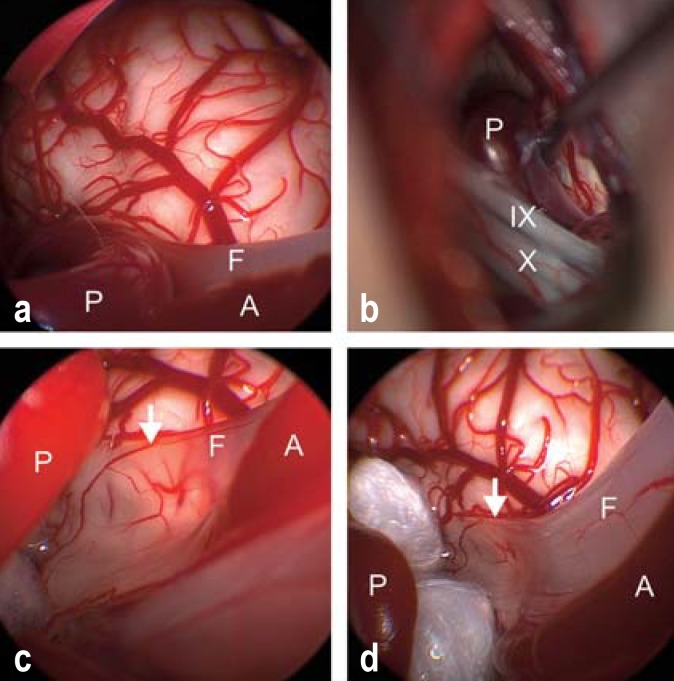
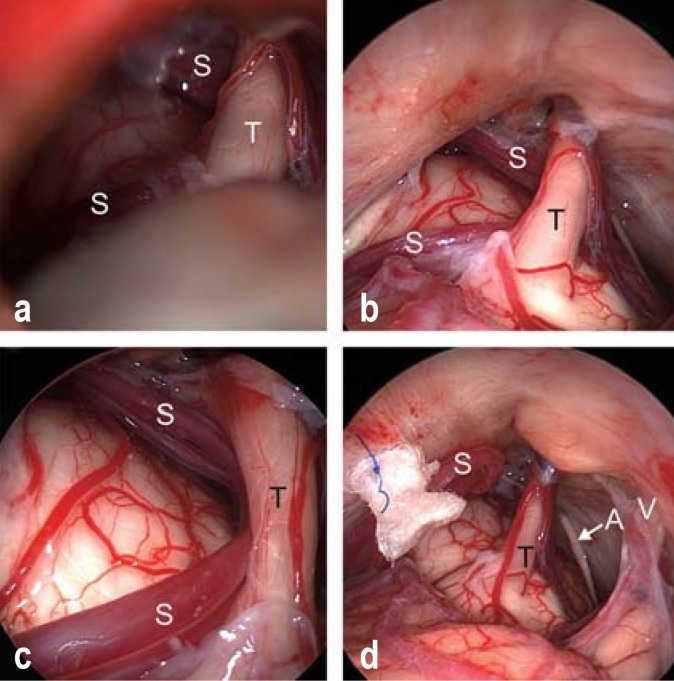
Results: These syndromes are caused by compression of a cranial nerve by an artery or vein at the zone of the nerve's entry to or exit from the brainstem. The best-known neurovascular compression syndrome is trigeminal neuralgia, followed by hemifacial spasm. Less well known are glossopharyngeal neuralgia, nervus intermedius neuralgia, and vestibular paroxysmia. The initial treatment of trigeminal neuralgia is medical: the first line of treatment is with sodium-blocking anticon- vulsants, such as carbamazepine. For patients with hemifacial spasm, botulinum toxin injection is the recommended initial treatment and often leads to a satisfactory regression of the spasms. If these treatments fail, a microvascular decompression operation is indicated. The aim of the procedure is to separate the irritating vessel from the nerve and to keep these structures apart permanently. There is hardly any available evidence on these treatment strategies from randomized controlled trials.
Conclusion: Nerve compression syndromes in the posterior cranial fossa can generally be treated nonsurgically at first. Over the course of the condition, however, treatment failure or intolerable side effects may arise. In such cases, a microvascu- lar decompression operation is indicated. This is a causally directed form of treat- ment that generally yields very good results.
Figures

References
-
- Donahue JH, Ornan DA, Mukherjee S. Imaging of vascular compression syndromes. Radiol Clin North Am. 2017;55:123–138. - PubMed
-
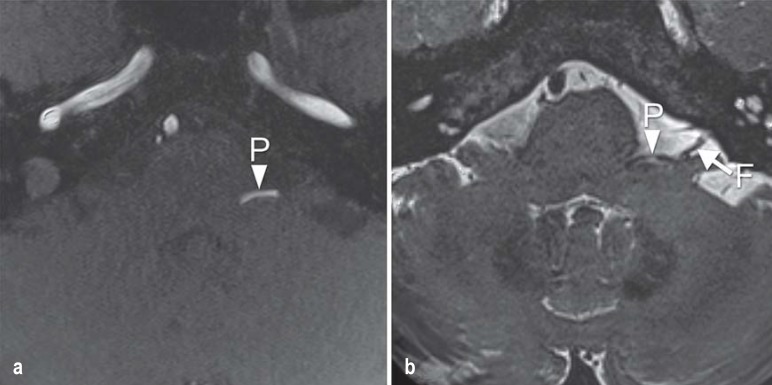
- El Refaee E, Langner S, Baldauf J, Matthes M, Kirsch M, Schroeder HW. Value of 3-dimensional high-resolution magnetic resonance imaging in detecting the offending vessel in hemifacial spasm: comparison with intraoperative high definition endoscopic visualization. Neurosurgery. 2013;73:58–67. - PubMed
-
- Katusic S, Williams DB, Beard CM, Bergstralh EJ, Kurland LT. Epidemiology and clinical features of idiopathic trigeminal neuralgia and glossopharyngeal neuralgia: similarities and differences Rochester, Minnesota, 1945-1984. Neuroepidemiology. 1991;10:276–281. - PubMed
-
- Manzoni GC, Torelli P. Epidemiology of typical and atypical craniofacial neuralgias. Neurol Sci. 2005;26(Suppl 2):s65–s67. - PubMed
-
- Fromm GH. Trigeminal neuralgia and related disorders. Neurol Clin. 1989;7:305–319. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous