

Continuous versus intermittent infusions of antibiotics for the treatment of infectious diseases: Meta-analysis and systematic review
- PMID: 30855448
- PMCID: PMC6417613
- DOI: 10.1097/MD.0000000000014632
Continuous versus intermittent infusions of antibiotics for the treatment of infectious diseases: Meta-analysis and systematic review
Abstract
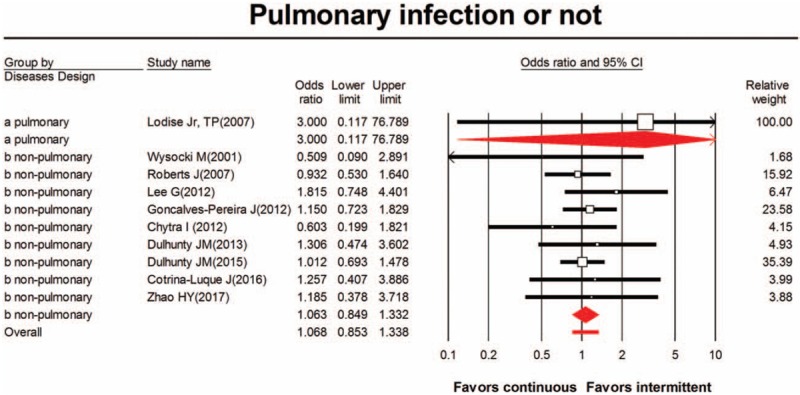
Background: Severe sepsis and pneumonia are common problems in the intensive care units (ICUs) and cause high morbidity and mortality. Optimal doses and appropriate routes of antibiotics are critical to improve their efficacy, but their appropriate routes remain controversial.
Objective: The efficacy of antibiotic administration among critically ill patient populations remains controversial. Therefore, the present meta-analysis aimed to investigate the effectiveness of antibiotic administration in patients with infection and to assess whether the effect differs between the two antibiotic administration types.
Methods: A systematic search of studies on continuous infusions of intravenous antibiotics and traditional intermittent infusions of antibiotics for patients with infection was performed mainly in PubMed. The odds ratios (ORs) of the microbiological results as primary outcome and mortality rate, length of stay, and duration of antibiotic treatment as secondary outcomes were evaluated.
Results: The meta-analysis comprised 9 randomized controlled trials (RCTs) and 4 retrospective studies comprising 1957 participants. Current analysis showed that the overall OR of clinical success between the continuous and intermittent groups was 0.675 (95% confidence interval [CI]: 0.523-0.870). Comparing continuous and intermittent groups, the subgroup analysis showed a lower ICU stay (OR 0.834, 95% CI: 0.542-1.282), a higher mortality (OR 1.433, 95% CI: 1.139-1.801), and a longer antibiotic duration (OR 1.055, 95% CI: 0.659-1.689), but the results of present meta-analysis were not significant because of the limited number of enrolled trials.
Limitations: Heterogeneity of included trials and studies.
Conclusions: The results of present meta-analysis were insufficient to recommend continuous infusion of intravenous antibiotics better than traditional intermittent infusions of antibiotics at routine clinical care. Hope large-scale RCT to provide more rebuts evidence for making recommendations to warrant continuous infusions of intravenous antibiotics at clinical practice.
Conflict of interest statement
All authors declare that they have no competing interests.
The authors have no conflicts of interest to disclose.
Figures








References
-
- Mandell LA, Wunderink RG. Kasper D, Fauci A, Hauser S, et al. Pneumonia. Harrison's Principles of Internal Medicine McGraw-Hill Education, 19th ednNew York, NY: 2015.
-
- Civitarese AM, Ruggieri E, Walz JM, et al. A 10-year review of total hospital-onset ICU bloodstream infections at an academic medical center. Chest 2017;151:1011–7. - PubMed
-
- Dellinger RP. The surviving sepsis campaign: 2013 and beyond. Chin Med J (Engl) 2013;126:1803–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
