

Fractures and Linear Growth in a Nationwide Cohort of Boys With Duchenne Muscular Dystrophy With and Without Glucocorticoid Treatment: Results From the UK NorthStar Database
- PMID: 30855644
- PMCID: PMC6563545
- DOI: 10.1001/jamaneurol.2019.0242
Fractures and Linear Growth in a Nationwide Cohort of Boys With Duchenne Muscular Dystrophy With and Without Glucocorticoid Treatment: Results From the UK NorthStar Database
Erratum in
-
Incorrectly Categorized Group Author.JAMA Neurol. 2019 Jun 1;76(6):732. doi: 10.1001/jamaneurol.2019.0904. JAMA Neurol. 2019. PMID: 30985878 Free PMC article. No abstract available.
-
Error in Abstract.JAMA Neurol. 2019 Jun 1;76(6):732. doi: 10.1001/jamaneurol.2019.1455. JAMA Neurol. 2019. PMID: 31180456 Free PMC article. No abstract available.
Abstract
Importance: Based on studies with relatively small sample size, fragility fractures are commonly reported in glucocorticoid (GC)-treated boys with Duchenne muscular dystrophy (DMD).
Objective: To determine the fracture burden and growth impairment in a large contemporary cohort of boys with DMD in the United Kingdom and in relation to GC regimen.
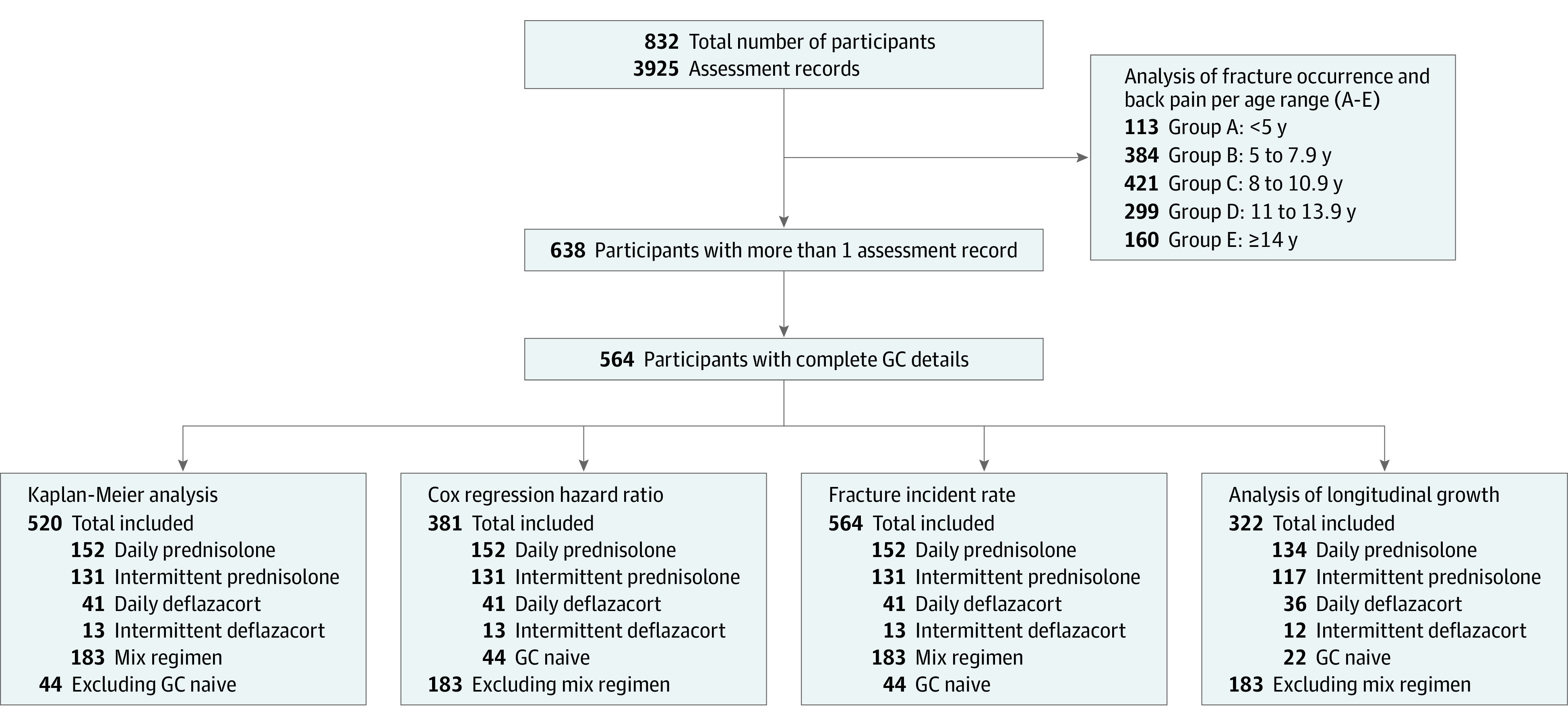
Design, setting, and participants: A retrospective review of fracture morbidity and growth from 832 boys with DMD in the UK NorthStar database (2006-2015), which systematically captures information from 23 participating centers. A total of 564 boys had more than 1 visit. No numbers of boys who refused were collected, but informal data from 2 centers in London and from Scotland show that refusal is very low. Data were analyzed between October 2006 and October 2015.
Main outcomes and measures: Fracture incidence rate per 10 000 person-years was determined. Cox regression analysis was used to identify factors associated with first fracture.
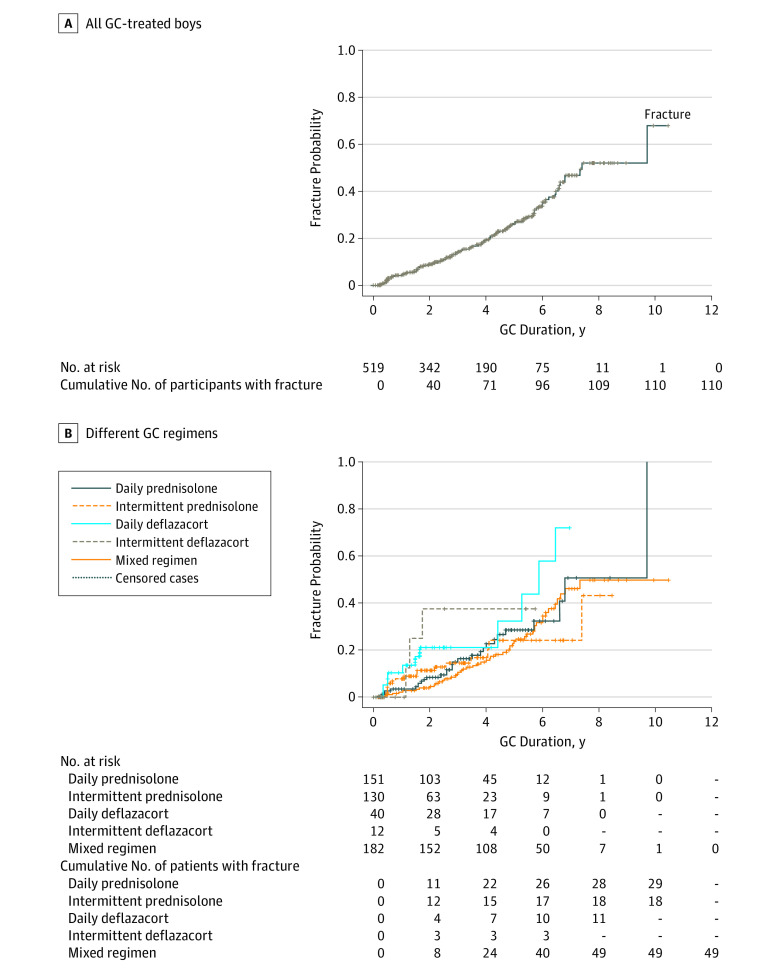
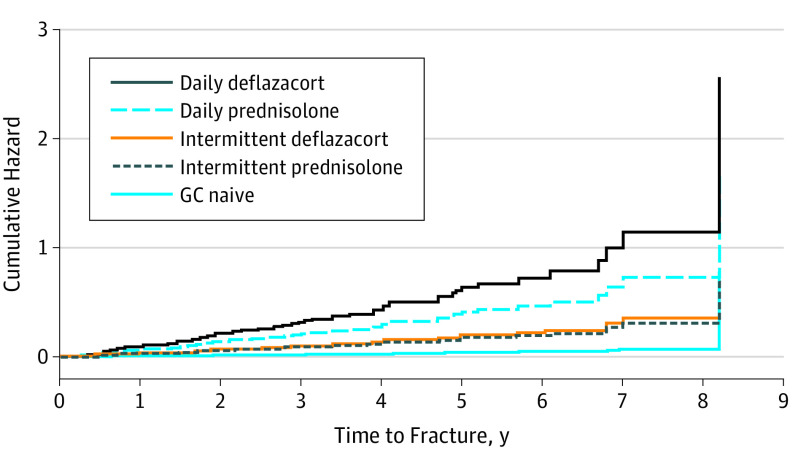
Results: Median age at baseline was 6.9 years (interquartile range, 4.9-7.2 years). At baseline, new fractures were reported in 7 of 564 participants (1.2%). During a median follow-up of 4 years (interquartile range, 2.0-6.0 years), incident fractures were reported in 156 of 564 participants (27.7%), corresponding to an overall fracture incidence rate of 682 per 10 000 person-years (95% CI, 579-798). The highest fracture incidence rate was observed in those treated with daily deflazacort at 1367 per 10 000 person-years (95% CI, 796-2188). After adjusting for age at last visit, mean hydrocortisone equivalent dose, mobility status, and bisphosphonate use prior to first fracture, boys treated with daily deflazacort had a 16.0-fold increased risk for first fracture (95% CI, 1.4-180.8; P = .03). Using adjusted regression models, change in height standard deviation scores was -1.6 SD lower (95% CI, -3.0 to -0.1; P = .03) in those treated with daily deflazacort compared with GC-naive boys, whereas there were no statistical differences in the other GC regimen.
Conclusions and relevance: In this large group of boys with DMD with longitudinal data, we document a high fracture burden. Boys treated with daily deflazacort had the highest fracture incidence rate and the greatest degree of linear growth failure. Clinical trials of primary bone protective therapies and strategies to improve growth in boys with DMD are urgently needed, but stratification based on GC regimen may be necessary.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
