

Patient Safety Outcomes under Flexible and Standard Resident Duty-Hour Rules
- PMID: 30855740
- PMCID: PMC6476299
- DOI: 10.1056/NEJMoa1810642
Patient Safety Outcomes under Flexible and Standard Resident Duty-Hour Rules
Abstract
Background: Concern persists that extended shifts in medical residency programs may adversely affect patient safety.
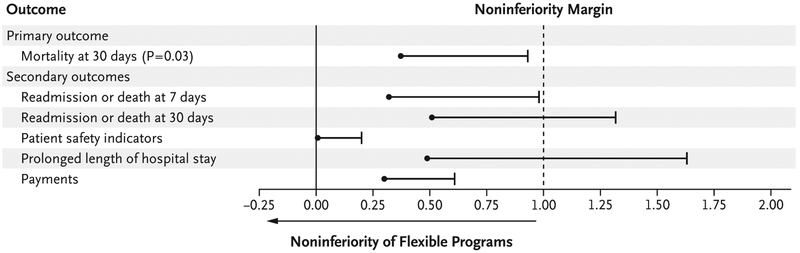
Methods: We conducted a cluster-randomized noninferiority trial in 63 internal-medicine residency programs during the 2015-2016 academic year. Programs underwent randomization to a group with standard duty hours, as adopted by the Accreditation Council for Graduate Medical Education (ACGME) in July 2011, or to a group with more flexible duty-hour rules that did not specify limits on shift length or mandatory time off between shifts. The primary outcome for each program was the change in unadjusted 30-day mortality from the pretrial year to the trial year, as ascertained from Medicare claims. We hypothesized that the change in 30-day mortality in the flexible programs would not be worse than the change in the standard programs (difference-in-difference analysis) by more than 1 percentage point (noninferiority margin). Secondary outcomes were changes in five other patient safety measures and risk-adjusted outcomes for all measures.
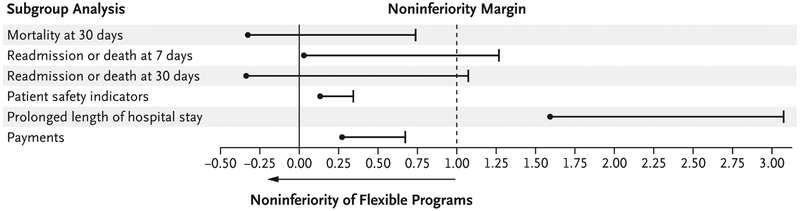
Results: The change in 30-day mortality (primary outcome) among the patients in the flexible programs (12.5% in the trial year vs. 12.6% in the pretrial year) was noninferior to that in the standard programs (12.2% in the trial year vs. 12.7% in the pretrial year). The test for noninferiority was significant (P = 0.03), with an estimate of the upper limit of the one-sided 95% confidence interval (0.93%) for a between-group difference in the change in mortality that was less than the prespecified noninferiority margin of 1 percentage point. Differences in changes between the flexible programs and the standard programs in the unadjusted rate of readmission at 7 days, patient safety indicators, and Medicare payments were also below 1 percentage point; the noninferiority criterion was not met for 30-day readmissions or prolonged length of hospital stay. Risk-adjusted measures generally showed similar findings.
Conclusions: Allowing program directors flexibility in adjusting duty-hour schedules for trainees did not adversely affect 30-day mortality or several other measured outcomes of patient safety. (Funded by the National Heart, Lung, and Blood Institute and Accreditation Council for Graduate Medical Education; iCOMPARE ClinicalTrials.gov number, NCT02274818.).
Copyright © 2019 Massachusetts Medical Society.
Figures
Comment in
-
Eyes Wide Open - Examining the Data on Duty-Hour Reform.N Engl J Med. 2019 Mar 7;380(10):969-970. doi: 10.1056/NEJMe1817497. N Engl J Med. 2019. PMID: 30855748 No abstract available.
-
Re: Patient Safety Outcomes under Flexible and Standard Resident Duty-Hour Rules.J Urol. 2019 Aug;202(2):201-202. doi: 10.1097/01.JU.0000559595.55535.10. Epub 2019 Jul 8. J Urol. 2019. PMID: 31063065 No abstract available.
-
Patient Safety under Flexible and Standard Duty-Hour Rules.N Engl J Med. 2019 Jun 13;380(24):2379-2380. doi: 10.1056/NEJMc1905064. N Engl J Med. 2019. PMID: 31189044 Free PMC article. No abstract available.
-
Patient Safety under Flexible and Standard Duty-Hour Rules.N Engl J Med. 2019 Jun 13;380(24):2380. doi: 10.1056/NEJMc1905064. N Engl J Med. 2019. PMID: 31189045 No abstract available.
-
Patient Safety under Flexible and Standard Duty-Hour Rules.N Engl J Med. 2019 Jun 13;380(24):2380-2381. doi: 10.1056/NEJMc1905064. N Engl J Med. 2019. PMID: 31189046 No abstract available.
References
-
- Meehan TP, Fine MJ, Krumholz HM, et al. Quality of care, process, and outcomes in elderly patients with pneumonia. JAMA 1997; 278: 2080–4. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous