

The PYY/Y2R-Deficient Mouse Responds Normally to High-Fat Diet and Gastric Bypass Surgery
- PMID: 30857366
- PMCID: PMC6471341
- DOI: 10.3390/nu11030585
The PYY/Y2R-Deficient Mouse Responds Normally to High-Fat Diet and Gastric Bypass Surgery
Abstract
Background/goals: The gut hormone peptide YY (PYY) secreted from intestinal L-cells has been implicated in the mechanisms of satiation via Y2-receptor (Y2R) signaling in the brain and periphery and is a major candidate for mediating the beneficial effects of bariatric surgery on appetite and body weight.
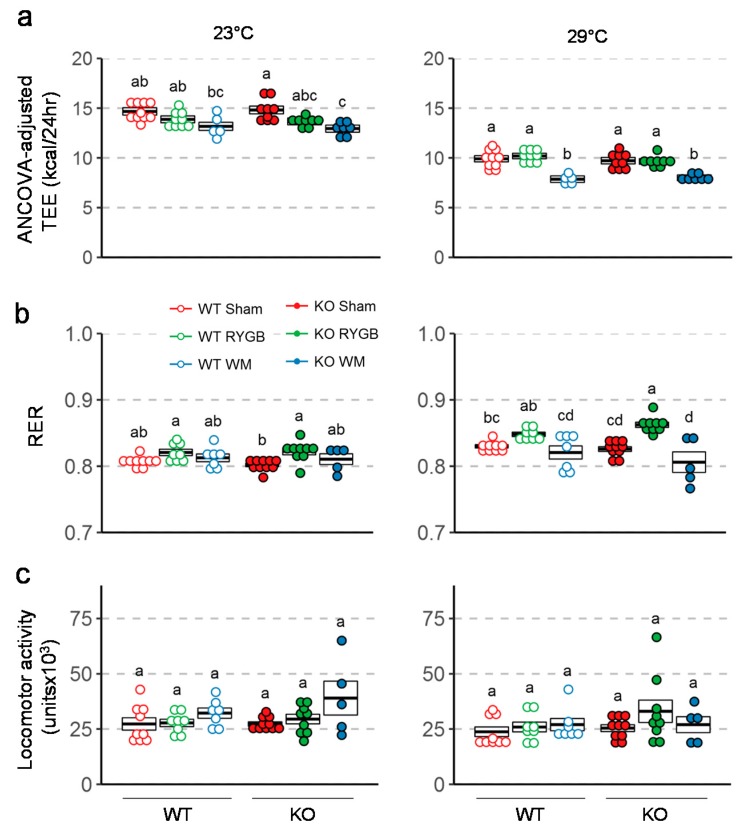
Methods: Here we assessed the role of Y2R signaling in the response to low- and high-fat diets and its role in the effects of Roux-en-Y gastric bypass (RYGB) surgery on body weight, body composition, food intake, energy expenditure and glucose handling, in global Y2R-deficient (Y2RKO) and wildtype (WT) mice made obese on high-fat diet.
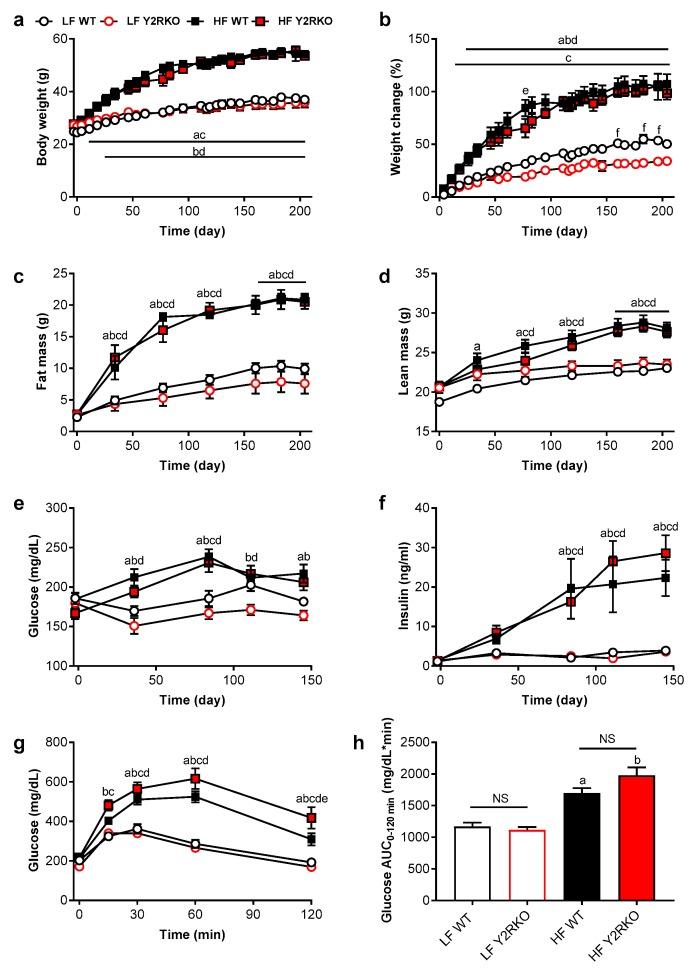
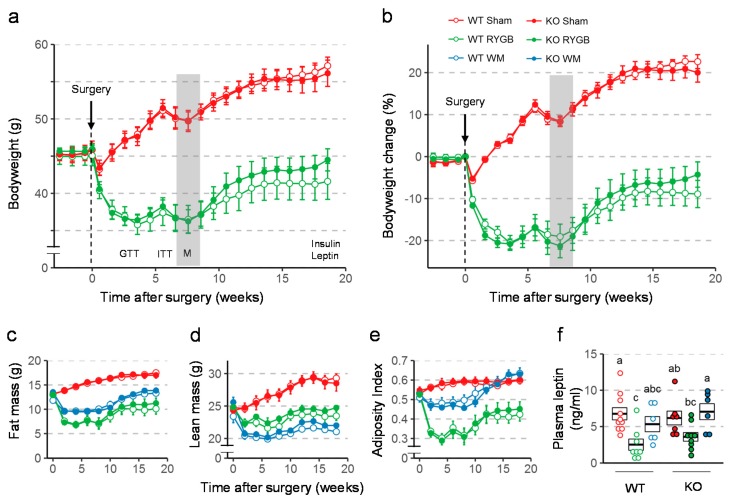
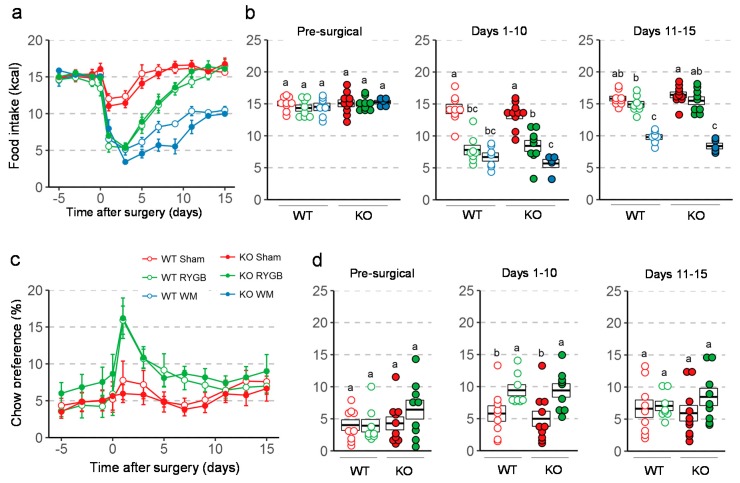
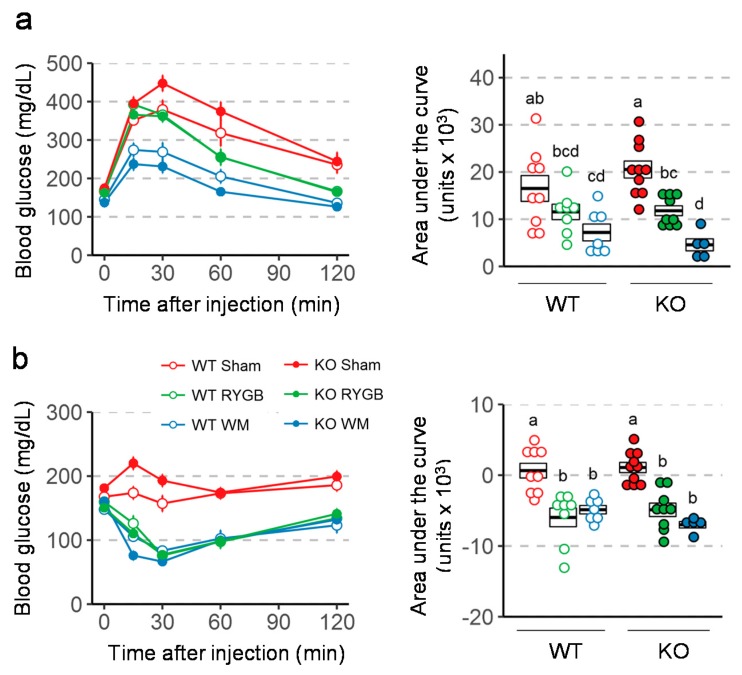
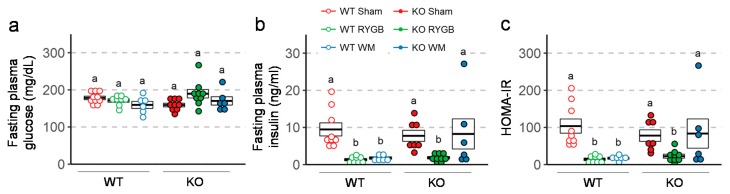
Results: Both male and female Y2RKO mice responded normally to low- and high-fat diet in terms of body weight, body composition, fasting levels of glucose and insulin, as well as glucose and insulin tolerance for up to 30 weeks of age. Contrary to expectations, obese Y2RKO mice also responded similarly to RYGB compared to WT mice for up to 20 weeks after surgery, with initial hypophagia, sustained body weight loss, and significant improvements in fasting insulin, glucose tolerance, insulin resistance (HOMA-IR), and liver weight compared to sham-operated mice. Furthermore, non-surgical Y2RKO mice weight-matched to RYGB showed the same improvements in glycemic control as Y2RKO mice with RYGB that were similar to WT mice.
Conclusions: PYY signaling through Y2R is not required for the normal appetite-suppressing and body weight-lowering effects of RYGB in this global knockout mouse model. Potential compensatory adaptations of PYY signaling through other receptor subtypes or other gut satiety hormones such as glucagon-like peptide-1 (GLP-1) remain to be investigated.
Keywords: body composition; body weight; diabetes; energy expenditure; glucose tolerance; incretin; insulin tolerance; obesity.
Conflict of interest statement
B.B., B.G., S.W., C.J.R. and J.L.T. are, or were at the time these studies were performed, employees and/or stockholders of MedImmune/AstraZeneca. None of the other authors declares any conflict of interest.
Figures
References
-
- Fisher D.P., Johnson E., Haneuse S., Arterburn D., Coleman K.J., O’Connor P.J., O’Brien R., Bogart A., Theis M.K., Anau J., et al. Association between bariatric surgery and macrovascular disease outcomes in patients with type 2 diabetes and severe obesity. JAMA. 2018;320:1570–1582. doi: 10.1001/jama.2018.14619. - DOI - PMC - PubMed
-
- Schauer P.R., Bhatt D.L., Kashyap S.R. bariatric surgery or intensive medical therapy for diabetes after 5 years. N. Engl. J. Med. 2018;376:1997. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
