

Assessing and monitoring the impact of the national newborn hearing screening program in Israel
- PMID: 30857547
- PMCID: PMC6410489
- DOI: 10.1186/s13584-019-0296-6
Assessing and monitoring the impact of the national newborn hearing screening program in Israel
Abstract
Background: The Israeli Newborn Hearing Screening Program (NHSP) began operating nationally in January 2010. The program includes the Otoacoustic Emissions (OAE) test for all newborns and Automated Auditory Brainstem Response (A-ABR) test for failed OAE and infants at risk for auditory neuropathy spectrum disorders. NHSP targets are diagnosis of hearing impairment by age three months and initiation of habilitation by six months.
Objectives: (1) Review NHSP coverage; (2) Assess NHSP impact on age at diagnosis for hearing impairment and age at initiation of habilitation; (3) Identify contributing factors and barriers to NHSP success.
Methods: (1) Analysis of screening coverage and referral rates for the NHSP; (2) Analysis of demographic data, results of coverage, age at diagnosis and initiation of habilitation for hearing impaired infants pre-implementation and post-implementation of NHSP from 10 habilitation centers; (3) Telephone interviews with parents whose infants failed the screening and were referred for further testing.
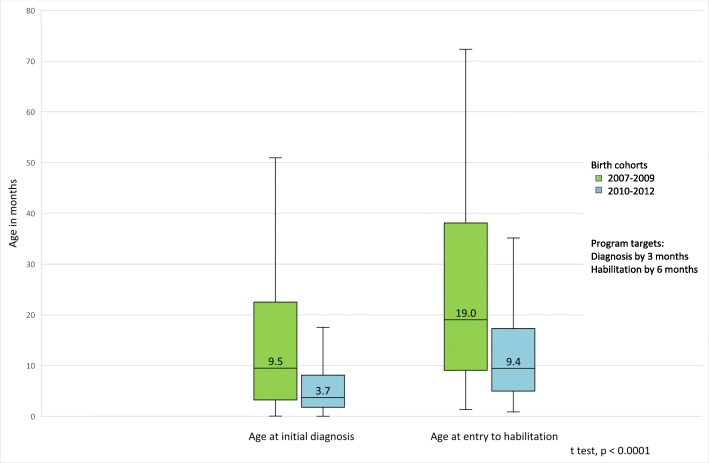
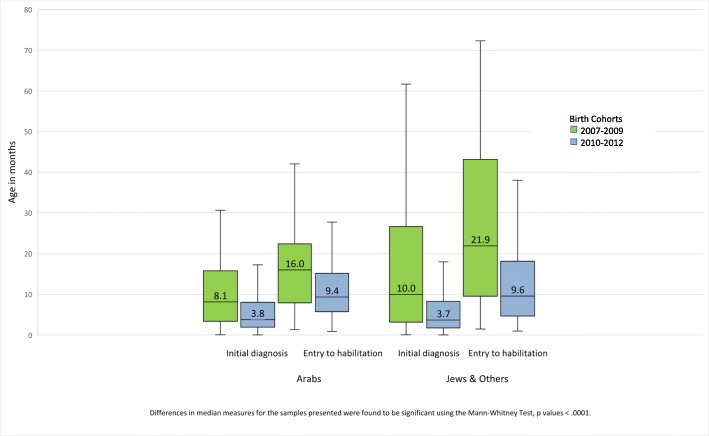
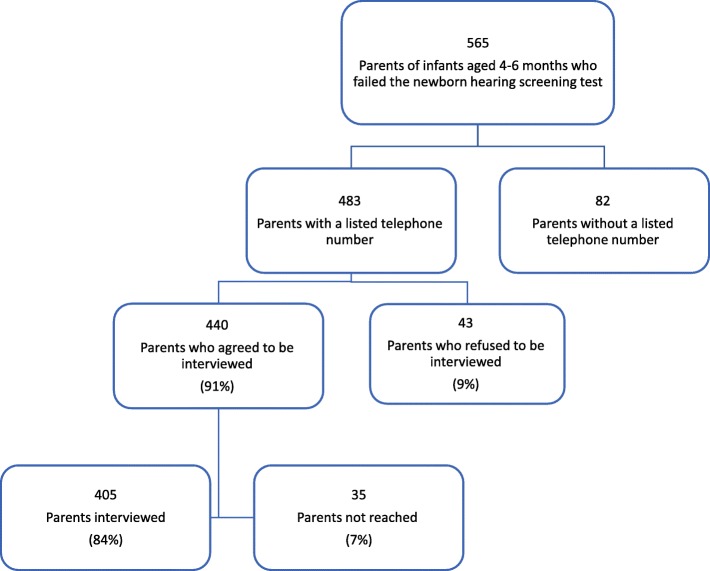
Results: The NHSP coverage was 98.7% (95.1 to 100%) for approximately 179,000 live births per year for 2014-2016 and average referral rates were under 3%. After three years of program implementation, median age at diagnosis was 3.7 months compared to 9.5 months prior to NHSP. The median age at initiation of habilitation after three years of NHSP was 9.4 months compared to 19.0 prior to NHSP. Parents (84% of 483 sampled) with infants aged 4-6 months participated in the telephone survey. While 84% of parents reported receiving a verbal explanation of the screening results, more than half of the parents reported not receiving written material. Parental report of understanding the test results and a heightened level of concern over the failed screen were associated with timely follow-up.
Conclusions: The findings indicate high screening coverage. The program reduced ages at diagnosis and initiation of habilitation for hearing impaired infants. Further steps needed to streamline the NHSP are improving communication among caregivers to parents to reduce anxiety; increasing efficiency in transferring information between service providers using advanced technology while ensuring continuum of care; reducing wait time for follow-up testing in order to meet program objectives. Establishment of a routine monitoring system is underway.
Keywords: Compliance; Congenital hearing loss; Early intervention; National public health program; Newborn hearing screening.
Conflict of interest statement
Ethics approval and consent to participate
Authorization was granted by the Ministry of Health’s Ethics Committee (No. 067/2011) to collect data from children’s charts at Habilitation Centers and recorded using a structured questionnaire. Anonymity of participants was retained by the use of coding therefore, consent to participate was waived.
Approval from the Ministry of Health’s Ethics Committee (No. 16/2015) was obtained in order to access computerized clinical health records of all government run MCHCs and conduct a telephone survey. Anonymity of participants was retained by the use of coding therefore, consent to participate was waived.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
