

Vasoactive-inotropic score and the prediction of morbidity and mortality after cardiac surgery
- PMID: 30857599
- PMCID: PMC6435836
- DOI: 10.1016/j.bja.2018.12.019
Vasoactive-inotropic score and the prediction of morbidity and mortality after cardiac surgery
Abstract
Background: The vasoactive-inotropic score (VIS) predicts mortality and morbidity after paediatric cardiac surgery. Here we examined whether VIS also predicted outcome in adults after cardiac surgery, and compared predictive capability between VIS and three widely used scoring systems.
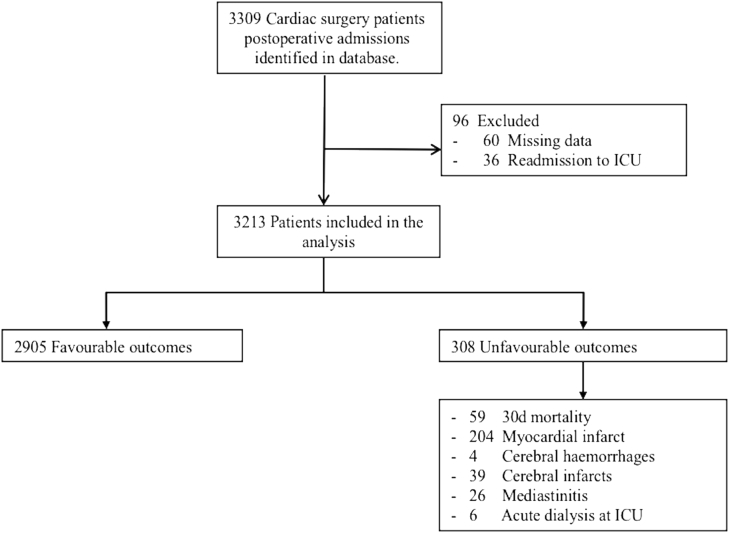
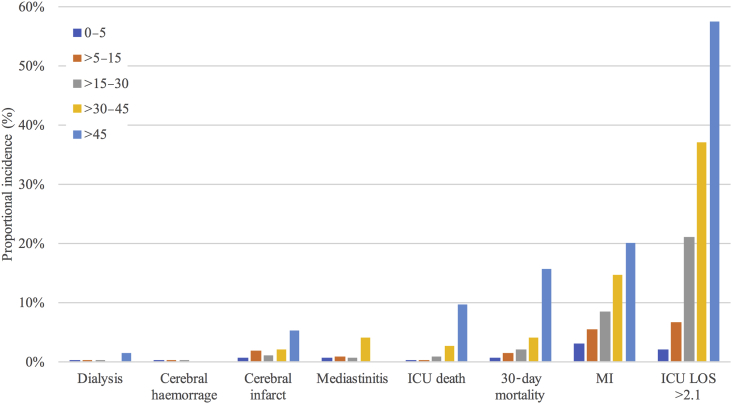
Methods: This single-centre retrospective cohort study included 3213 cardiac surgery patients. Maximal VIS (VISmax) was calculated using the highest doses of vasoactive and inotropic medications administered during the first 24 h post-surgery. We established five VISmax categories: 0-5, >5-15, >15-30, >30-45, and >45 points. The predictive accuracy of VISmax was evaluated for a composite outcome, which included 30-day mortality, mediastinitis, stroke, acute kidney injury, and myocardial infarction.
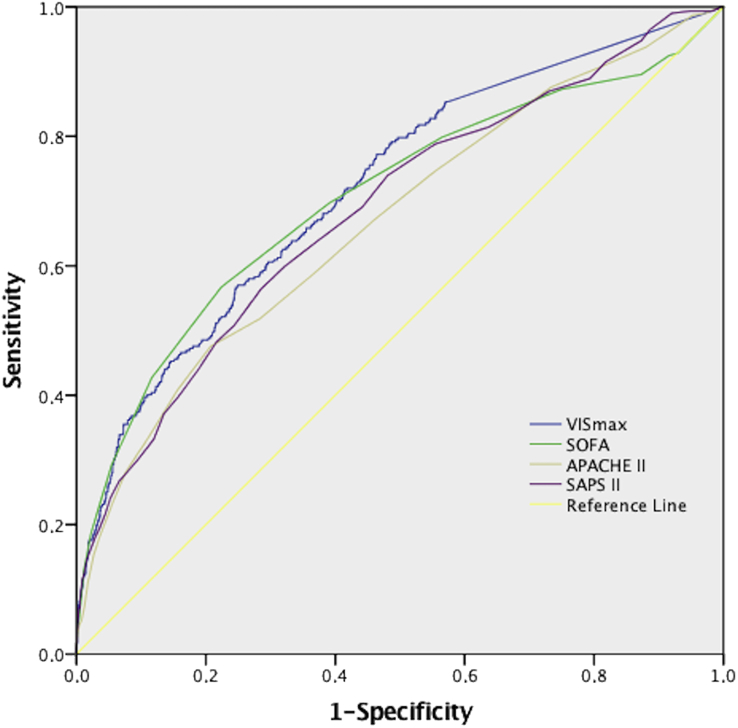
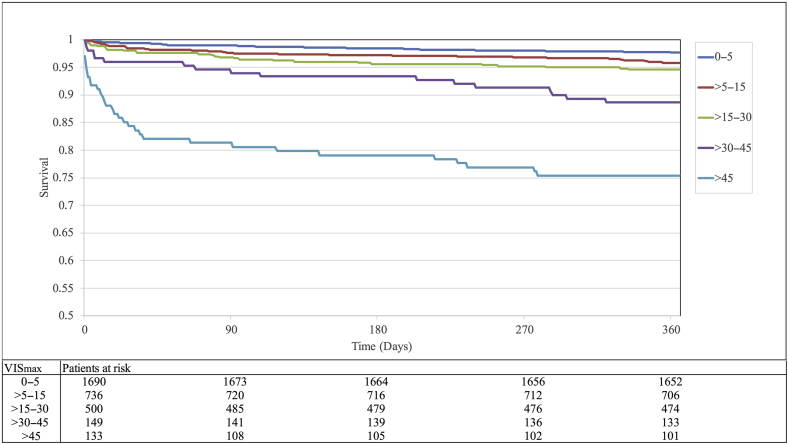
Results: VISmax showed good prediction accuracy for the composite outcome [area under the curve (AUC), 0.72; 95% confidence interval (CI), 0.69-0.75]. The incidence of the composite outcome was 9.6% overall and 43% in the highest VISmax group (>45). VISmax predicted 30-day mortality (AUC, 0.76; 95% CI, 0.69-0.83) and 1-yr mortality (AUC, 0.70; 95% CI, 0.65-0.74). Prediction accuracy for unfavourable outcome was significantly better with VISmax than with Acute Physiology and Chronic Health Evaluation II (P=0.01) and Simplified Acute Physiological Score II (P=0.048), but not with the Sequential Organ Failure Assessment score (P=0.32).
Conclusions: In adults after cardiac surgery, VISmax predicted a composite of unfavourable outcomes and predicted mortality up to 1 yr after surgery.
Keywords: acute kidney injury; cardiac surgery; cardiovascular system; mortality; myocardial infarction; postoperative outcome; risk assessment scoring system; stroke.
Copyright © 2019 British Journal of Anaesthesia. Published by Elsevier Ltd. All rights reserved.
Figures
References
-
- Doerr F., Badreldin A., Can F., Bayer O., Wahlers T., Hekmat K. SAPS 3 is not superior to SAPS 2 in cardiac surgery patients. Scand Cardiovasc J. 2014;48:111–119. - PubMed
-
- Vincent J.L., Moreno R., Takala J. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Aorking Group on Sepsis-related problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;22:707–710. - PubMed
-
- Knaus W.A., Draper E.A., Wagner D.P., Zimmerman J.E. APACHE II: a severity disease classification system. Crit Care Med. 1985;13:818–829. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
