

Postoperative critical care and high-acuity care provision in the United Kingdom, Australia, and New Zealand
- PMID: 30857602
- PMCID: PMC6435907
- DOI: 10.1016/j.bja.2018.12.026
Postoperative critical care and high-acuity care provision in the United Kingdom, Australia, and New Zealand
Abstract
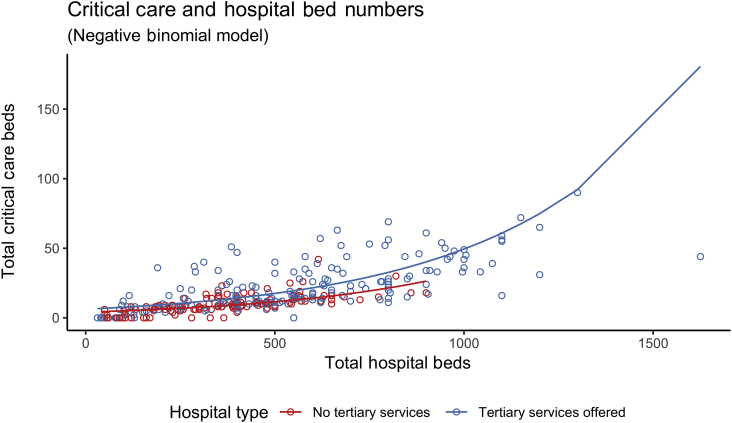
Background: Decisions to admit high-risk postoperative patients to critical care may be affected by resource availability. We aimed to quantify adult ICU/high-dependency unit (ICU/HDU) capacity in hospitals from the UK, Australia, and New Zealand (NZ), and to identify and describe additional 'high-acuity' beds capable of managing high-risk patients outside the ICU/HDU environment.
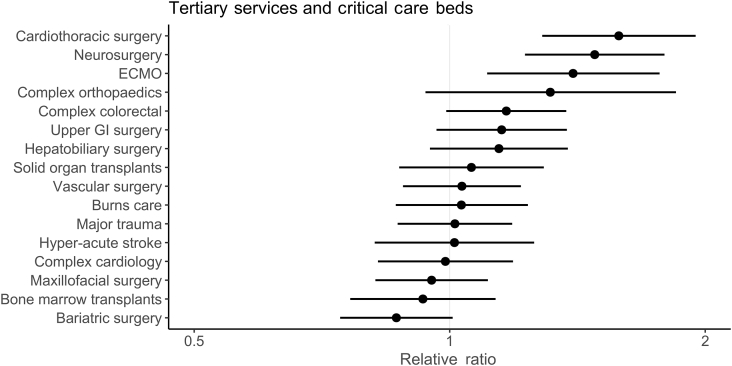
Methods: We used a modified Delphi consensus method to design a survey that was disseminated via investigator networks in the UK, Australia, and NZ. Hospital- and ward-level data were collected, including bed numbers, tertiary services offered, presence of an emergency department, ward staffing levels, and the availability of critical care facilities.
Results: We received responses from 257 UK (response rate: 97.7%), 35 Australian (response rate: 32.7%), and 17 NZ (response rate: 94.4%) hospitals (total 309). Of these hospitals, 91.6% reported on-site ICU or HDU facilities. UK hospitals reported fewer critical care beds per 100 hospital beds (median=2.7) compared with Australia (median=3.7) and NZ (median=3.5). Additionally, 31.1% of hospitals reported having high-acuity beds to which high-risk patients were admitted for postoperative management, in addition to standard ICU/HDU facilities. The estimated numbers of critical care beds per 100 000 population were 9.3, 14.1, and 9.1 in the UK, Australia, and NZ, respectively. The estimated per capita high-acuity bed capacities per 100 000 population were 1.2, 3.8, and 6.4 in the UK, Australia, and NZ, respectively.
Conclusions: Postoperative critical care resources differ in the UK, Australia, and NZ. High-acuity beds may have developed to augment the capacity to deliver postoperative critical care.
Keywords: critical care; health services research; patient safety; perioperative care; postoperative complications.
Copyright © 2019 British Journal of Anaesthesia. Published by Elsevier Ltd. All rights reserved.
Figures
References
-
- The Royal College of Anaesthetists . The Royal College of Anaesthetists; 2015. Perioperative medicine: the pathway to better surgical care.https://www.rcoa.ac.uk/sites/default/files/PERIOP-2014.pdf [accessed: 04 Jan 2018]
-
- Weiser T.G., Haynes A.B., Molina G. Estimate of the global volume of surgery in 2012: an assessment supporting improved health outcomes. Lancet. 2015;385:S11. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
