

Immunotherapy Is Changing First-Line Treatment of Metastatic Renal-Cell Carcinoma
- PMID: 30858035
- PMCID: PMC7004481
- DOI: 10.1016/j.clgc.2019.01.017
Immunotherapy Is Changing First-Line Treatment of Metastatic Renal-Cell Carcinoma
Abstract
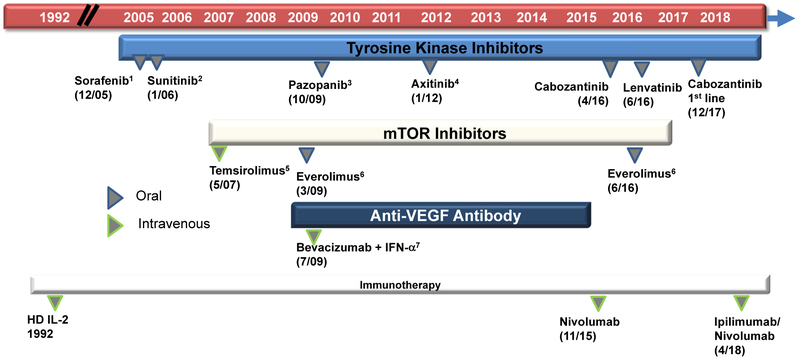
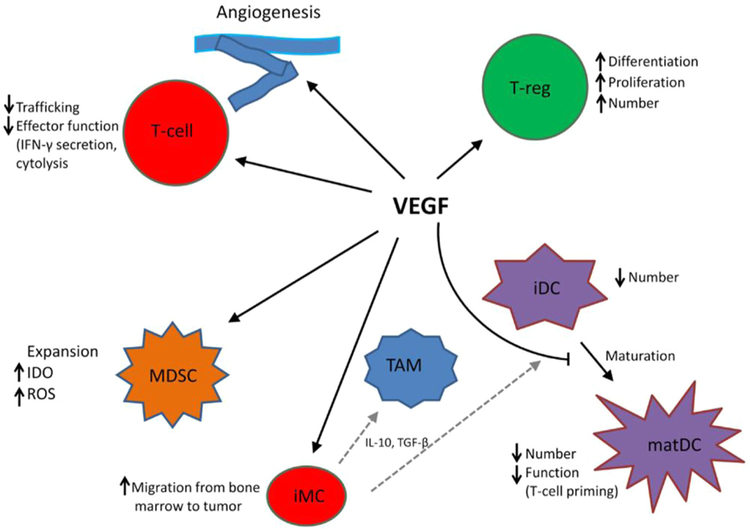
The incidence of renal-cell carcinoma has been increasing each year, with nearly one third of new cases diagnosed at advanced or metastatic stage. The advent of targeted therapies for metastatic renal-cell carcinoma (mRCC) has underscored the need to subtype tumors according to tumor-immune expression profiles that may more reliably predict treatment outcomes. Over the past 2 decades, several vascular endothelial growth factor (VEGF) and tyrosine kinase inhibitors have been the mainstay for first- and second-line treatment of mRCC. Very recently, immunotherapy checkpoint inhibitors have significantly changed the treatment landscape for patients with mRCC, particularly for first-line treatment of intermediate to poor risk mRCC patients. Now, combination immunotherapy as well as combinations of immunotherapy with targeted agents can significantly alter disease outcomes. The field of immuno-oncology for mRCC has unveiled a deeper understanding of the immunoreactivity inherent to these tumors, and as a result combination therapy is evolving as a first-line modality. This review provides a timeline of advances and controversies in first-line treatment of mRCC, describes recent advances in understanding the immunoreactivity of these tumors, and addresses the future of combination anti-VEGF and immunotherapeutic platforms.
Keywords: Immune checkpoint inhibitors; Metastatic renal-cell carcioma; Targeted therapies; VEGF therapies; VEGF-immunotherapy combinations.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure
A.J.A. has received funding (to Duke) from Medivation/Astellas, Bayer, Dendreon, Janssen, Active Biotech, Sanofi-Aventis, Gilead, Novartis, and Pfizer; consulting/speaking with Dendreon and Sanofi Aventis; and consulting with Medivation/Astellas and Janssen. D.J.G. has received research funding (to Duke) from Acerta, Astellas, Bayer, Bristol-Myers Squibb, Dendreon, Exelixis, Innocrin, Janssen, Novartis, Pfizer; consulting and speaking with Bayer, Exelixis, Sanofi; and consulting with Astellas, AstraZeneca, Bristol-Myers Squibb, Innocrin, Janssen, Merck, Myovant, Pfizer. T.Z. has received research funding (to Duke) from Pfizer, Janssen, Acerta, Abbvie, Novartis, Merrimack, OmniSeq, PGDx, and Merck; consulting/speaking with Genentech Roche and Exelixis; consulting with AstraZeneca, Amgen, Pharmacyclics, BMS, Pfizer, Foundation Medicine, Janssen, Bayer, and Sanofi Aventis; and stock ownership/employment (spouse) from Capio Biosciences. M.M. has received research funding (to Duke) from Janssen, Agensys, Bayer, Seattle Genetics, and Clovis. The other authors have stated that they have no conflict of interest.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin 2015; 65:5–29. - PubMed
-
- Motzer RJ, Agarwal N, Beard C, et al. Kidney cancer. J Natl Compr Canc Netw 2011; 9:960–77. - PubMed
-
- Fisher R, Gore M, Larkin J. Current and future systemic treatments for renal cell carcinoma. Semin Cancer Biol 2013; 23:38–45. - PubMed
-
- Climent MA, Munoz-Langa J, Basterretxea-Badiola L, et al. Systematic review and survival meta-analysis of real world evidence on first-line pazopanib for metastatic renal cell carcinoma. Crit Rev Oncol Hematol 2018; 121:45–50. - PubMed
-
- Vachhani P, George S. VEGF inhibitors in renal cell carcinoma. Clin Adv Hematol Oncol 2016; 14:1016–28. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
