

Relevance of Titin Missense and Non-Frameshifting Insertions/Deletions Variants in Dilated Cardiomyopathy
- PMID: 30858397
- PMCID: PMC6412046
- DOI: 10.1038/s41598-019-39911-x
Relevance of Titin Missense and Non-Frameshifting Insertions/Deletions Variants in Dilated Cardiomyopathy
Erratum in
-
Publisher Correction: Relevance of Titin Missense and Non-Frameshifting Insertions/Deletions Variants in Dilated Cardiomyopathy.Sci Rep. 2020 Oct 9;10(1):17264. doi: 10.1038/s41598-020-73763-0. Sci Rep. 2020. PMID: 33037269 Free PMC article.
Abstract
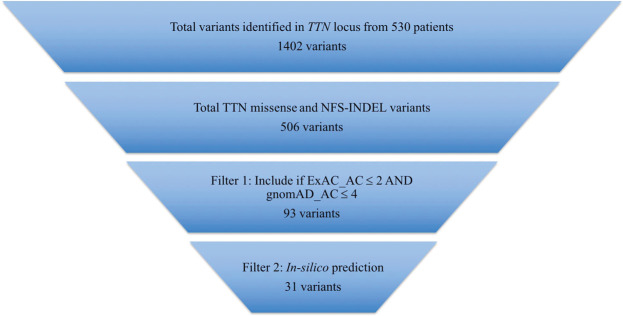
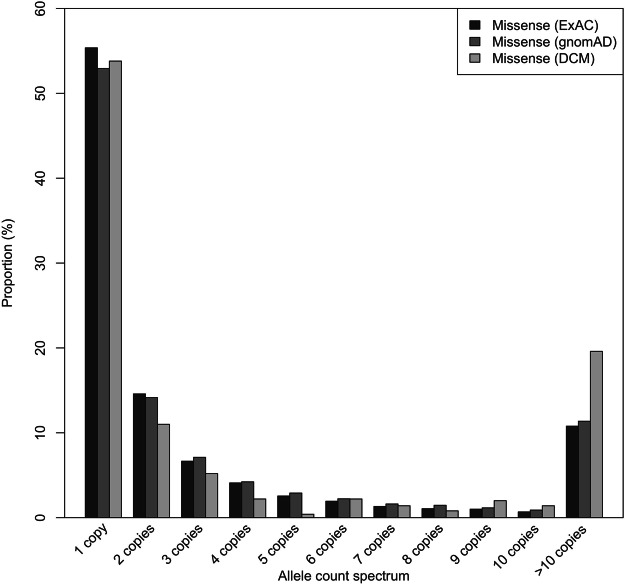
Recent advancements in next generation sequencing (NGS) technology have led to the identification of the giant sarcomere gene, titin (TTN), as a major human disease gene. Truncating variants of TTN (TTNtv) especially in the A-band region account for 20% of dilated cardiomyopathy (DCM) cases. Much attention has been focused on assessment and interpretation of TTNtv in human disease; however, missense and non-frameshifting insertions/deletions (NFS-INDELs) are difficult to assess and interpret in clinical diagnostic workflow. Targeted sequencing covering all exons of TTN was performed on a cohort of 530 primary DCM patients from three cardiogenetic centres across Europe. Using stringent bioinformatic filtering, twenty-nine and two rare TTN missense and NFS-INDELs variants predicted deleterious were identified in 6.98% and 0.38% of DCM patients, respectively. However, when compared with those identified in the largest available reference population database, no significant enrichment of such variants was identified in DCM patients. Moreover, DCM patients and reference individuals had comparable frequencies of splice-region missense variants with predicted splicing alteration. DCM patients and reference populations had comparable frequencies of rare predicted deleterious TTN missense variants including splice-region missense variants suggesting that these variants are not independently causative for DCM. Hence, these variants should be classified as likely benign in the clinical diagnostic workflow, although a modifier effect cannot be excluded at this stage.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
