

Causal associations of blood lipids with risk of ischemic stroke and intracerebral hemorrhage in Chinese adults
- PMID: 30858617
- PMCID: PMC6795549
- DOI: 10.1038/s41591-019-0366-x
Causal associations of blood lipids with risk of ischemic stroke and intracerebral hemorrhage in Chinese adults
Abstract
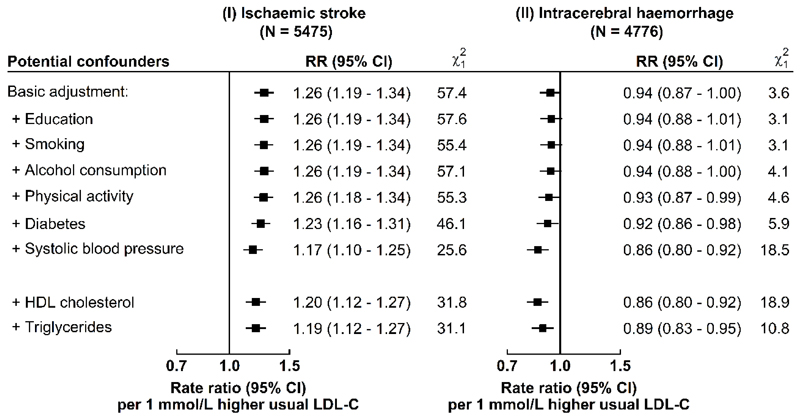
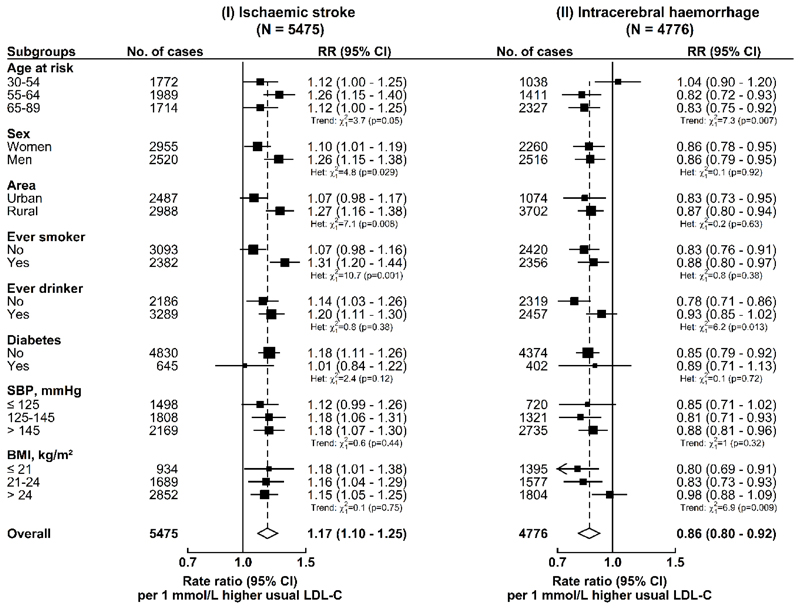
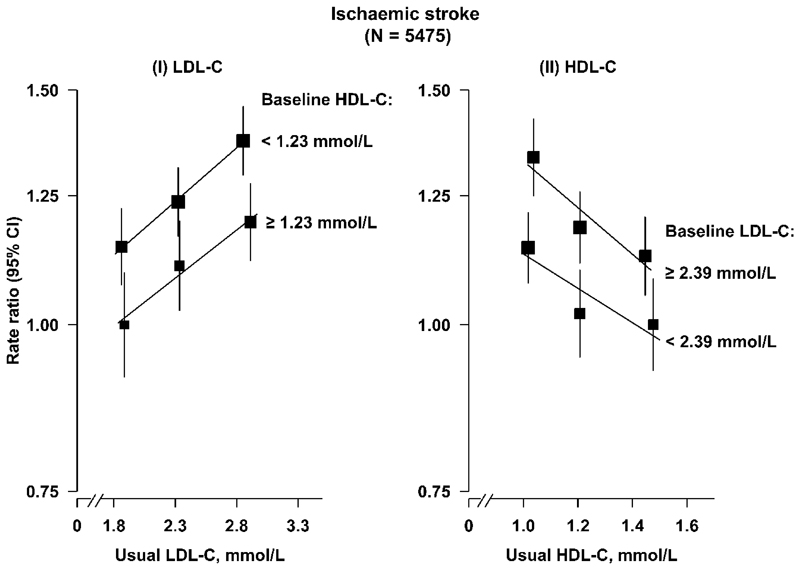
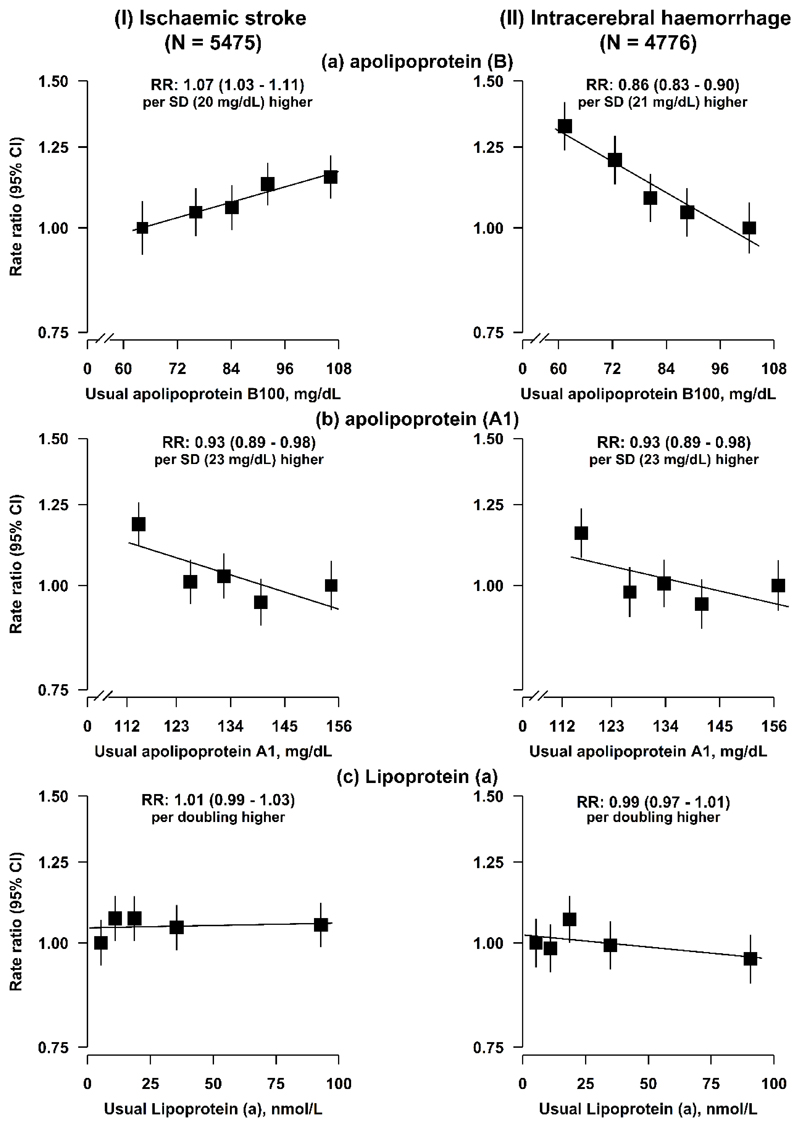
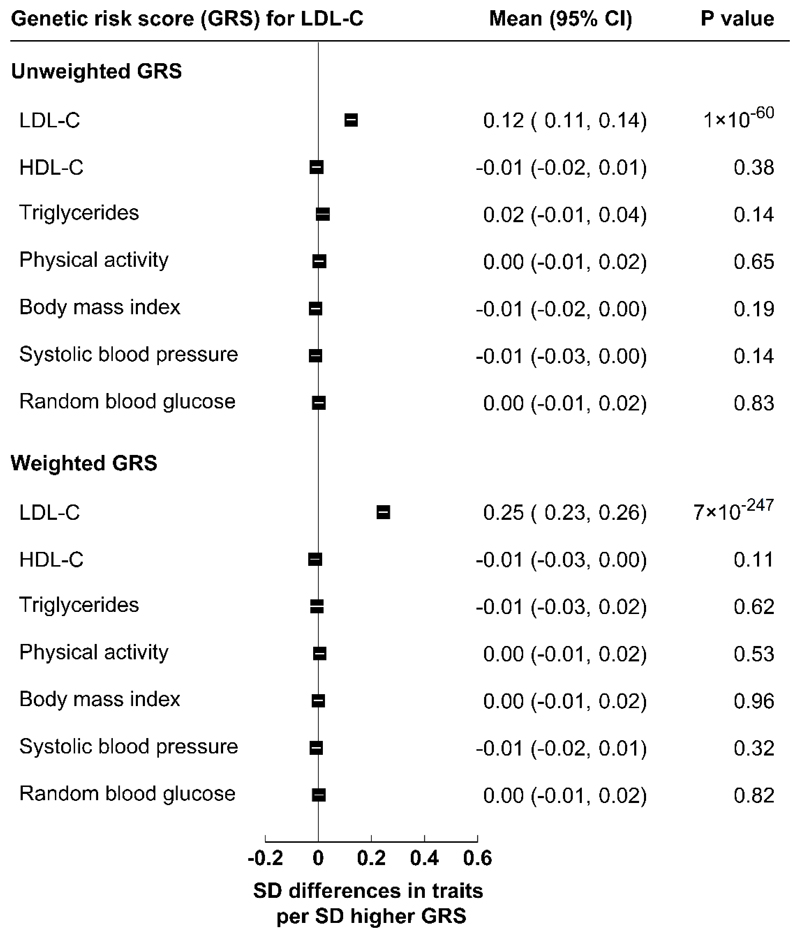
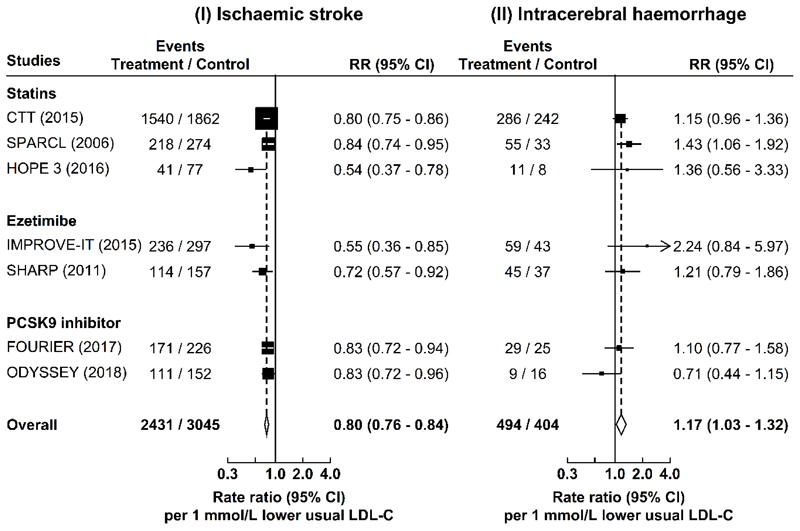
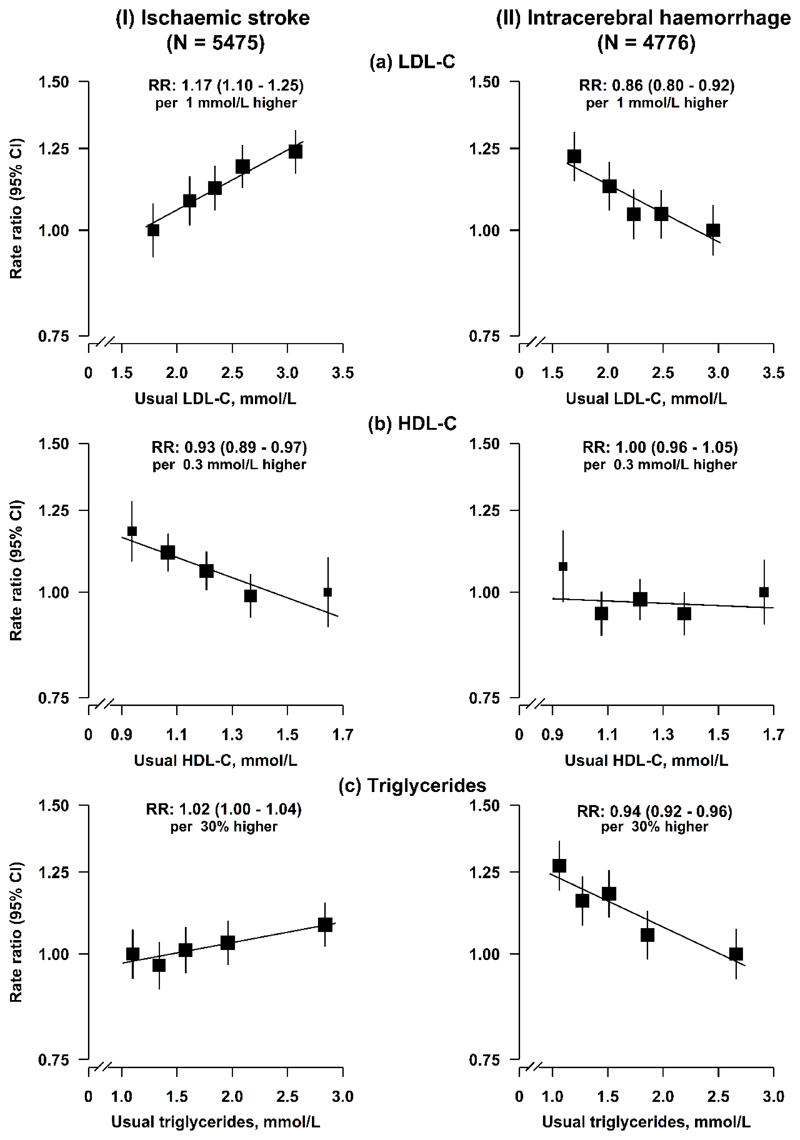
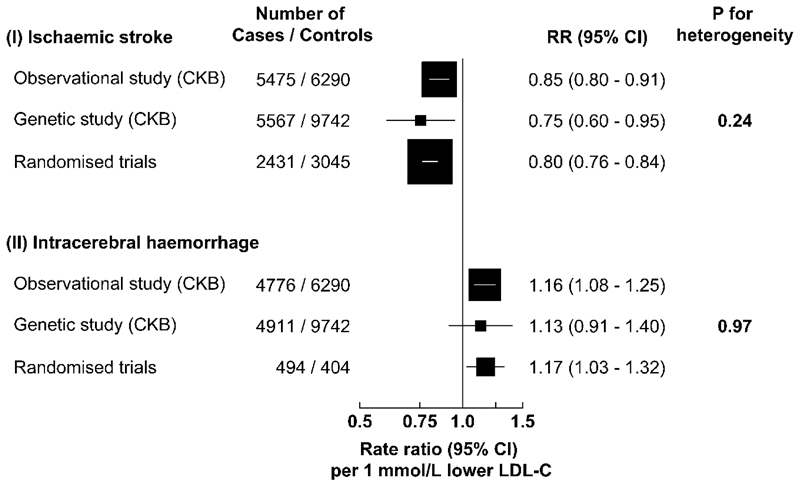
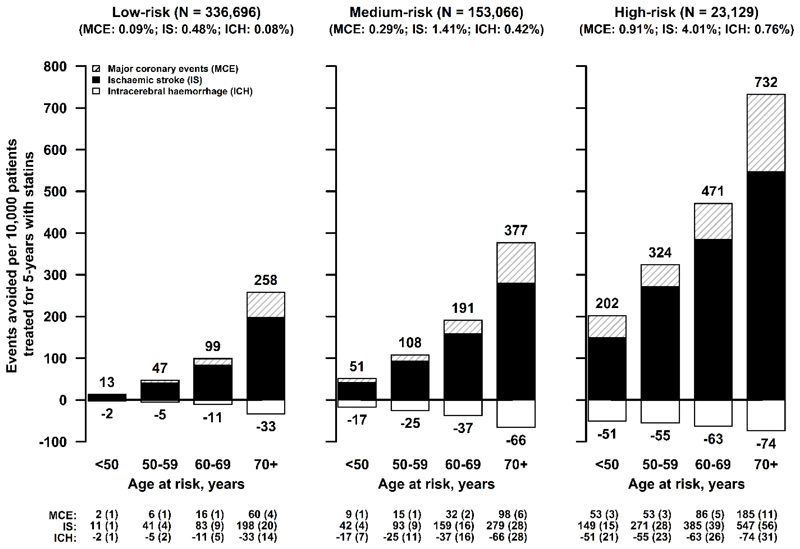
Stroke is the second leading cause of death worldwide and accounts for >2 million deaths annually in China1,2. Ischemic stroke (IS) and intracerebral hemorrhage (ICH) account for an equal number of deaths in China, despite a fourfold greater incidence of IS1,2. Stroke incidence and ICH proportion are higher in China than in Western populations3-5, despite having a lower mean low-density lipoprotein cholesterol (LDL-C) concentration. Observational studies reported weaker positive associations of LDL-C with IS than with coronary heart disease (CHD)6,7, but LDL-C-lowering trials demonstrated similar risk reductions for IS and CHD8-10. Mendelian randomization studies of LDL-C and IS have reported conflicting results11-13, and concerns about the excess risks of ICH associated with lowering LDL-C14,15 may have prevented the more widespread use of statins in China. We examined the associations of biochemically measured lipids with stroke in a nested case-control study in the China Kadoorie Biobank (CKB) and compared the risks for both stroke types associated with equivalent differences in LDL-C in Mendelian randomization analyses. The results demonstrated positive associations of LDL-C with IS and equally strong inverse associations with ICH, which were confirmed by genetic analyses and LDL-C-lowering trials. Lowering LDL-C is still likely to have net benefit for the prevention of overall stroke and cardiovascular disease in China.
Conflict of interest statement
Figures
Comment in
-
Divergent effects of lipids on stroke.Nat Med. 2019 Apr;25(4):543-544. doi: 10.1038/s41591-019-0413-7. Nat Med. 2019. PMID: 30911137 No abstract available.
-
Lipid lowering and risk of haemorrhagic stroke in CKD.Nat Rev Nephrol. 2019 Nov;15(11):667-669. doi: 10.1038/s41581-019-0201-0. Nat Rev Nephrol. 2019. PMID: 31467442 No abstract available.
References
-
- Global Burden of Disease Study 2016. Global Burden of Disease Study 2016 (GBD 2016) Results. Seattle, United States: Institute for Health Metrics and Evaluation (IHME); 2016.
-
- Zhou M, et al. Cause-specific mortality for 240 causes in China during 1990-2013: a systematic subnational analysis for the Global Burden of Disease Study 2013. Lancet. 2015;387:251–272. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- MC_U137686851/MRC_/Medical Research Council/United Kingdom
- RG/18/13/33946/BHF_/British Heart Foundation/United Kingdom
- RG/13/13/30194/BHF_/British Heart Foundation/United Kingdom
- 212946/Z/18/Z/WT_/Wellcome Trust/United Kingdom
- 212946/WT_/Wellcome Trust/United Kingdom
- MC_PC_14135/MRC_/Medical Research Council/United Kingdom
- MC_UU_00017/1/MRC_/Medical Research Council/United Kingdom
- MC_U137686855/MRC_/Medical Research Council/United Kingdom
- MC_UU_12026/2/MRC_/Medical Research Council/United Kingdom
- 202922/WT_/Wellcome Trust/United Kingdom
- MC_PC_13049/MRC_/Medical Research Council/United Kingdom
- 088158/WT_/Wellcome Trust/United Kingdom
- 104085/WT_/Wellcome Trust/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
