

Improvement of Deep Brain Stimulation in Dyskinesia in Parkinson's Disease: A Meta-Analysis
- PMID: 30858823
- PMCID: PMC6397831
- DOI: 10.3389/fneur.2019.00151
Improvement of Deep Brain Stimulation in Dyskinesia in Parkinson's Disease: A Meta-Analysis
Abstract
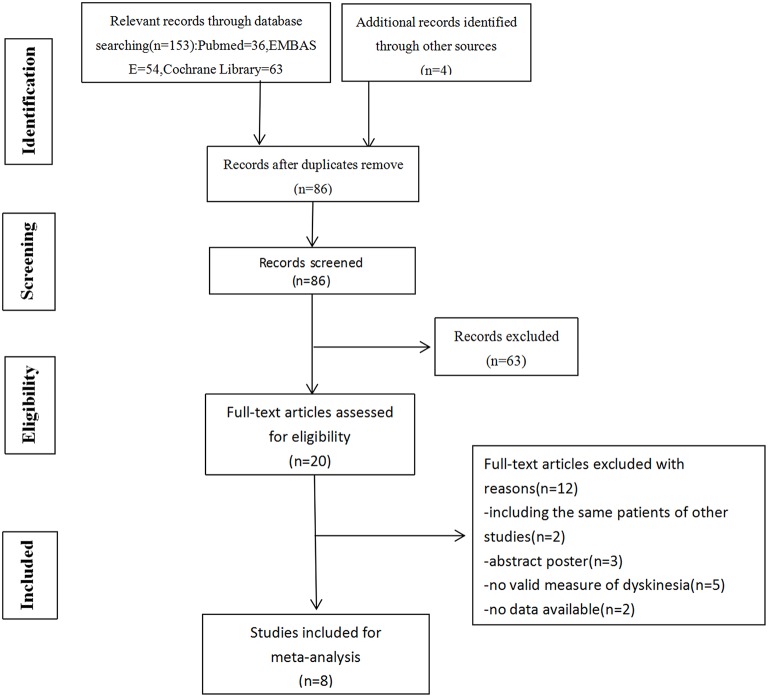
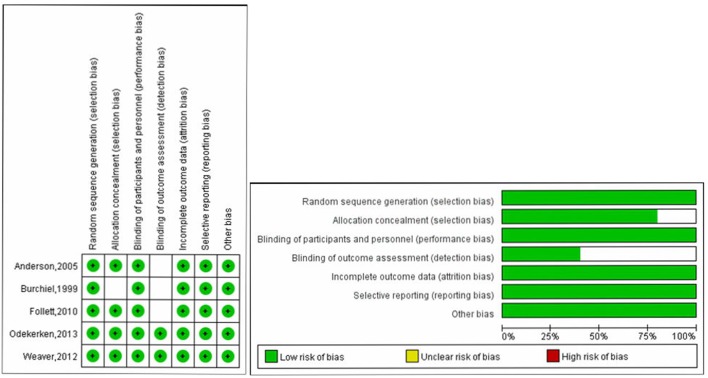
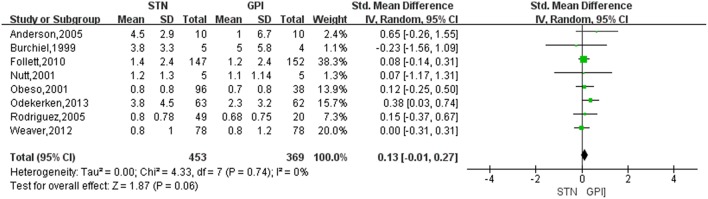
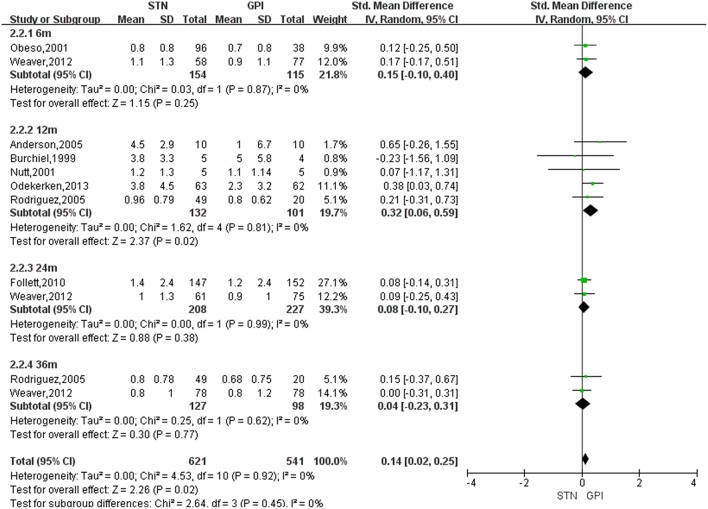
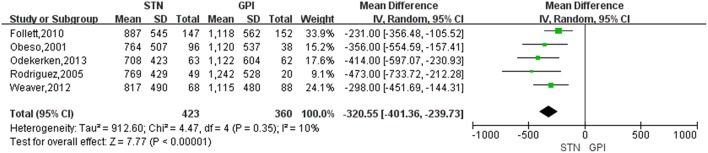
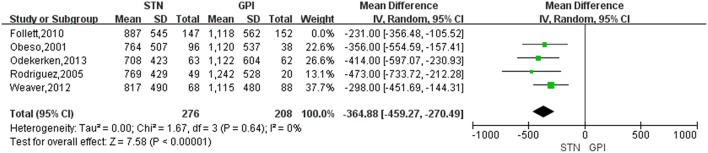
Background: Deep brain stimulation (DBS) of the subthalamic nucleus (STN) or globus pallidus internus (GPi) have been proven to be equally effective in improving motor-symptoms for advanced Parkinson's disease (PD) patients. However, it is unclear that which target stimulation is more effective in reducing dyskinesia. We conducted the meta-analysis to evaluate the efficacy of STN and GPi-DBS in the dyskinesia. Methods: A systematic search was performed in PubMed, Embase, and the Cochrane Library databases. Controlled trials about the dyskinesia comparing the efficacy of GPi and STN DBS were included. Clinical data of dyskinesia and levodopa equivalent doses (LED) were collected for the meta-analysis. Results: Eight eligible trials containing a total of 822 patients were included in this meta-analysis. Our results showed that GPi DBS offered a greater reduction of dyskinesia than STN DBS at 12 months after surgery, with an overall pooled SMD of 0.32 (95% CI = 0.06 to 0.59, P = 0.02). Treatment of STN DBS was associated with a greater reduction of LED compared with GPi DBS, with a change score of -320.55 (95% CI = -401.36 to -239.73, P < 0.00001). Conclusion: GPi DBS is superior to reduce dyskinesia than STN DBS at 12 months after surgery for advanced PD patients. Further studies should focus on the different mechanism for dyskinesia reduction by GPi or STN DBS.
Keywords: Parkinson's disease; deep brain stimulation; dyskinesia; globus pallidus interna; subthalamic nucleus.
Figures
References
-
- Iansek R, Centre K, Victoria C. Pharmacological management of Parkinson's disease. J Pharm Pract Res. (2004) 34:229–32. 10.1002/jppr2004343229 - DOI
Publication types
LinkOut - more resources
Full Text Sources