

Who to Test for Hepatitis C Virus in the Middle East and North Africa?: Pooled Analyses of 2,500 Prevalence Measures, Including 49 Million Tests
- PMID: 30859146
- PMCID: PMC6396361
- DOI: 10.1002/hep4.1310
Who to Test for Hepatitis C Virus in the Middle East and North Africa?: Pooled Analyses of 2,500 Prevalence Measures, Including 49 Million Tests
Abstract
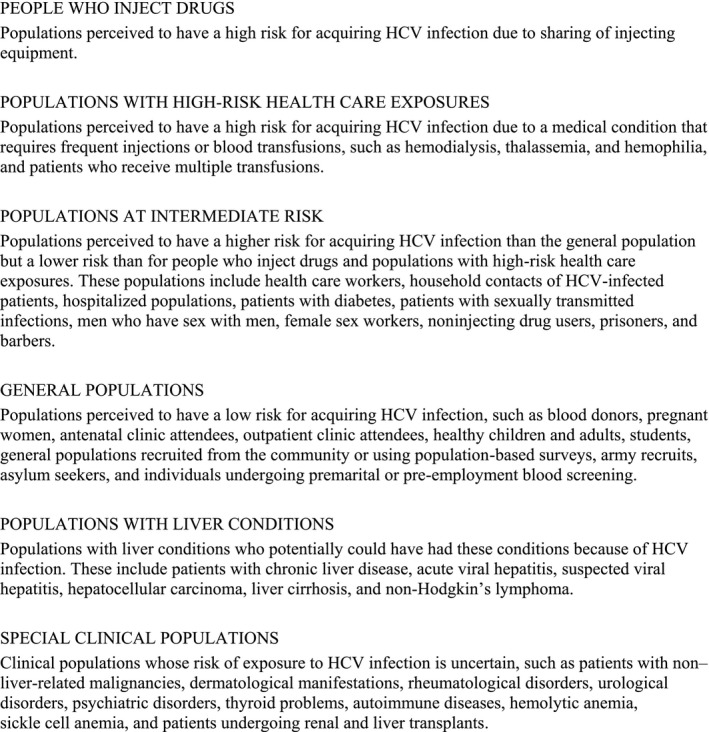
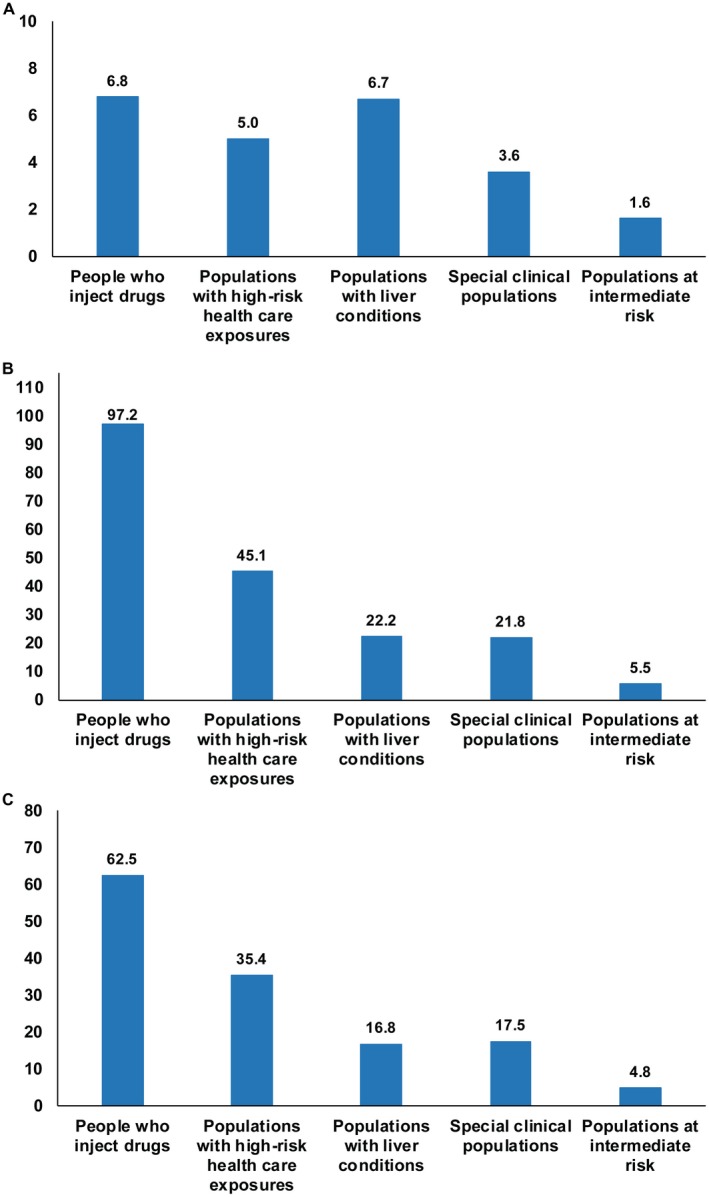
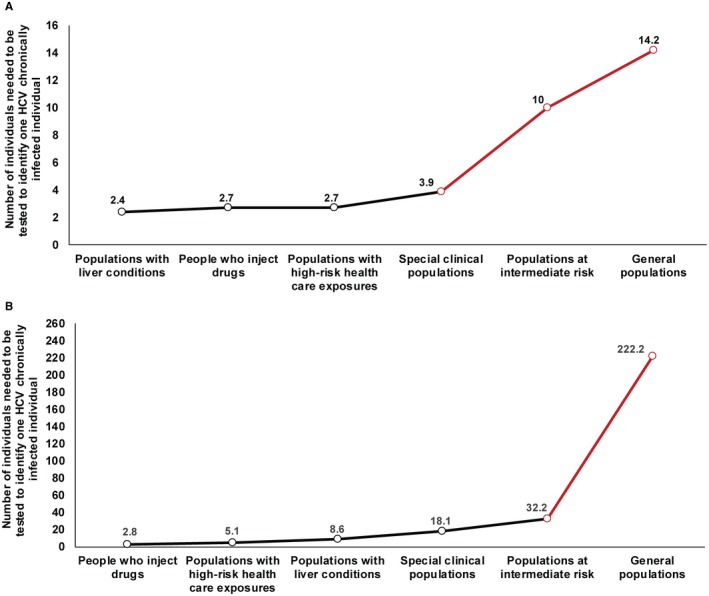
Expanding hepatitis C virus (HCV) treatment coverage is challenged by limited testing and diagnosis. This study assessed the risk of exposure, for the Middle East and North Africa, by population, yields of testing, and program efficiency of testing strategies. A standardized and systematically assembled database of 2,542 HCV antibody prevalence studies on 49 million individuals was analyzed. Random effects meta-analyses were conducted to estimate pooled measures for risk of exposure, risk ratio (RR) of exposure, and yields of testing. Program expansion path curves were calculated to assess program efficiency. Countries clustered into two patterns: generalized versus concentrated epidemics. In generalized epidemics (Egypt and Pakistan) relative to general populations, RR of exposure was 6.8 for people who inject drugs (PWID), 6.7 for populations with liver conditions, and 5.0 for populations with high-risk health care exposures. In concentrated epidemics (remaining countries), corresponding RRs were 97.2, 45.1, and 22.2, respectively. In generalized epidemics, the number of tests needed to identify a chronic infection was 2.5 for PWID, 2.4 for populations with liver conditions, 2.7 for populations with high-risk health care exposures, and 14.2 for general populations. In concentrated epidemics, corresponding numbers were 2.8, 8.6, 5.1, and 222.2, respectively. Program expansion path curves demonstrated major gains in program efficiency by targeting specific populations. Risk of exposure varies immensely by population and shows a distinctive hierarchy, particularly in concentrated epidemics. Testing strategies can be much more efficient through population prioritization by risk of exposure. General population testing is not programmatically efficient in concentrated epidemics.
Figures
References
-
- Mohd Hanafiah K, Groeger J, Flaxman AD, Wiersma ST. Global epidemiology of hepatitis C virus infection: new estimates of age‐specific antibody to HCV seroprevalence. Hepatology 2013;57:1333‐1342. - PubMed
-
- Lavanchy D. Evolving epidemiology of hepatitis C virus. Clin Microbiol Infect 2011;17:107‐115. - PubMed
-
- World Health Organization . The Global Hepatitis Report. Geneva, Switzerland: World Health Organization; 2017.
-
- Gower E, Estes C, Blach S, Razavi‐Shearer K, Razavi H. Global epidemiology and genotype distribution of the hepatitis C virus infection. J Hepatol 2014;61(Suppl.):S45‐S57. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
