

Transoral endoscopic thyroidectomy using vestibular approach: A single center experience
- PMID: 30860079
- PMCID: PMC6515781
- DOI: 10.4103/jpgm.JPGM_117_18
Transoral endoscopic thyroidectomy using vestibular approach: A single center experience
Abstract
Background: Thyroid Natural Orifice Transluminal Endoscopic Surgery (NOTES) or transoral endoscopic thyroidectomy using vestibular approach is a recent advance embraced by the surgical community because of its potential for a scar-free thyroidectomy. In this article, we present our initial experience with this technique.
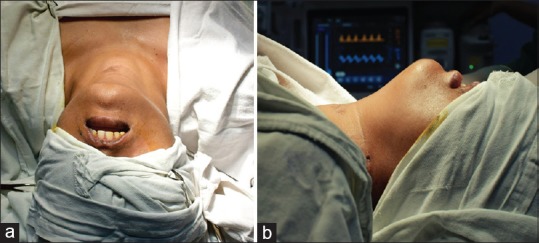
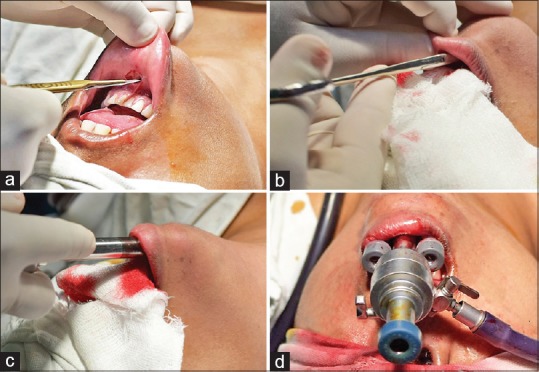
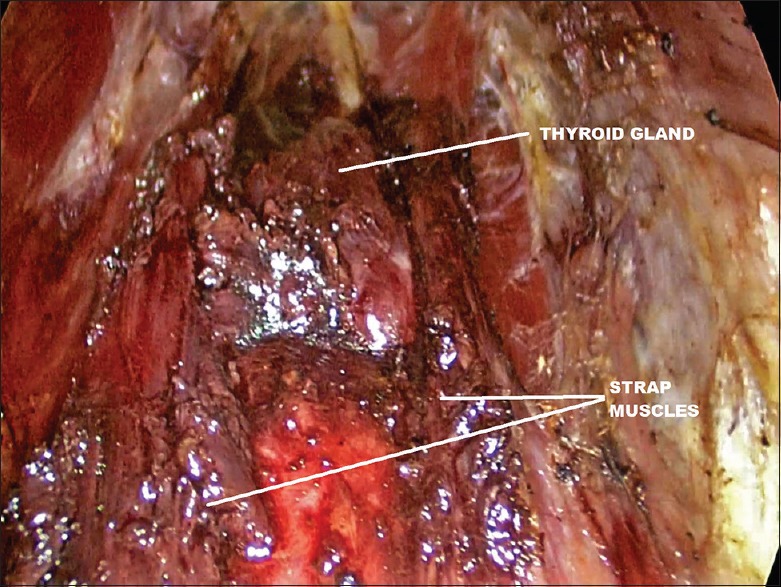
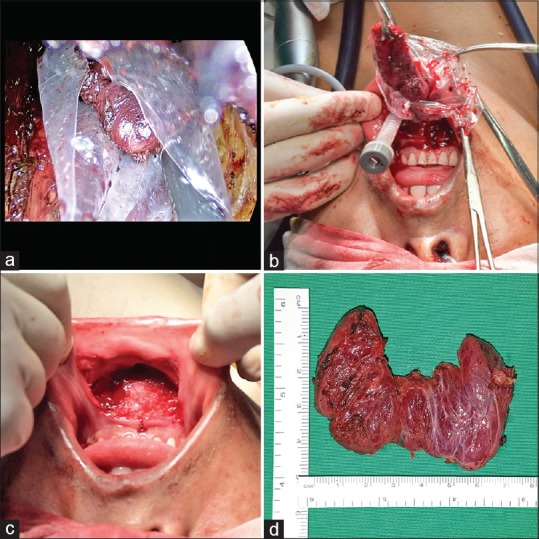
Materials and methods: We used a three-port technique through the oral vestibule, one 10 mm port for the laparoscope and two additional 5 mm ports for the endoscopic instruments required. The carbon dioxide insufflation pressure was set at 12 mm of Hg. Anterior cervical subplatysmal space was created from the oral vestibule down to the sternal notch, and the thyroidectomy was done using conventional laparoscopic instruments and a harmonic scalpel.
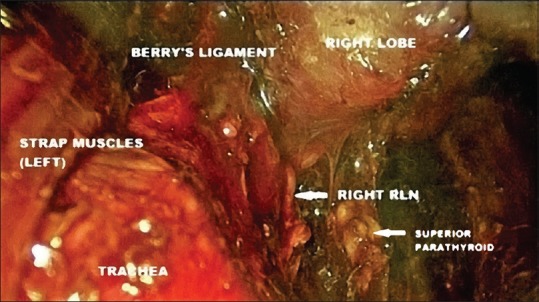
Results: From May 2016 to December 2017, we have performed ten such procedures in the Department of General Surgery in our hospital, which is a tertiary referral center. Six patients had solitary thyroid nodules, for which a hemi-thyroidectomy was done. Four patients had multi-nodular goiter and total thyroidectomy or near-total thyroidectomy was done. The preoperative fine-needle aspiration cytology (FNAC) was suggestive of Bethesda class 2 lesions in all the patients with multinodular goiter and in five of the six patients with solitary nodular goiter. Only one patient with solitary nodular goiter had a Bethesda class 3 lesion on FNAC. The final histopathological report of the specimen was benign, either colloid goiter, or degenerative nodule in all cases of multinodular goiter and in four cases of solitary thyroid nodule. In one Bethesda class 2 solitary nodule, the histopathological report was suggestive of follicular carcinoma; in the Bethesda class 3 solitary nodule, the histopathological report was suggestive of follicular variant of papillary carcinoma. No complication such as temporary or permanent vocal cord paralysis, hypoparathyroidism, subcutaneous emphysema, pneumomediastinum, tracheal injury, esophageal injury, mental nerve palsy, or surgical site infection was found postoperatively. However, two patients developed small hematomas in the midline.
Conclusion: Transoral endoscopic thyroidectomy is a safe, feasible, and minimally invasive technique with excellent cosmetic results.
Keywords: Endoscopic thyroidectomy using vestibular approach; scar.free thyroidectomy; transoral endoscopic thyroidectomy.
Conflict of interest statement
None
Figures

Comment in
-
Transoral thyroidectomy- Breaking new grounds??J Postgrad Med. 2019 Apr-Jun;65(2):72-73. doi: 10.4103/jpgm.JPGM_91_19. J Postgrad Med. 2019. PMID: 31036777 Free PMC article. No abstract available.
References
-
- Wong K, Lang B. Endoscopic thyroidectomy: A literature review and update. Curr Surg Rep. 2013;1:7–15.
-
- Witzel K, von Rahden BH, Kaminski C, Stein HJ. Transoral access for endoscopic thyroid resection. Surg Endosc. 2008;22:1871–5. - PubMed
-
- Tan CT, Cheah WK, Delbridge L. “Scar less” (in the neck) endoscopic thyroidectomy (SET): An evidence-based review of published techniques. World J Surg. 2008;32:1349–57. - PubMed
-
- Philip WS, Laura RH, Leslie JS, John BH. Thyroid. In: Townsend C, Evers B, Mattox K, Beauchamp R, editors. Sabiston Textbook of Surgery. Philadelphia: Elsevier; 2017. pp. 881–922.
-
- Anuwong A. Transoral endoscopic thyroidectomy vestibular approach: A series of the first 60 human cases. World J Surg. 2016;40:491–7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical