

TBCRC 022: A Phase II Trial of Neratinib and Capecitabine for Patients With Human Epidermal Growth Factor Receptor 2-Positive Breast Cancer and Brain Metastases
- PMID: 30860945
- PMCID: PMC6494354
- DOI: 10.1200/JCO.18.01511
TBCRC 022: A Phase II Trial of Neratinib and Capecitabine for Patients With Human Epidermal Growth Factor Receptor 2-Positive Breast Cancer and Brain Metastases
Abstract
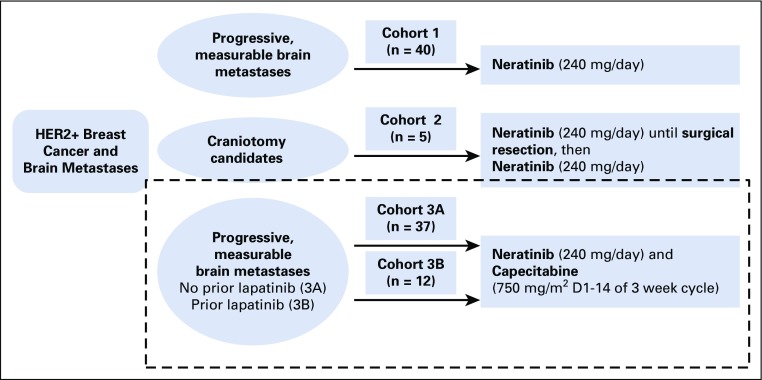
Purpose: Evidence-based treatments for metastatic, human epidermal growth factor receptor 2 (HER2)-positive breast cancer to the CNS are limited. We previously reported modest activity of neratinib monotherapy for HER2-positive breast cancer brain metastases. Here we report the results from additional study cohorts.
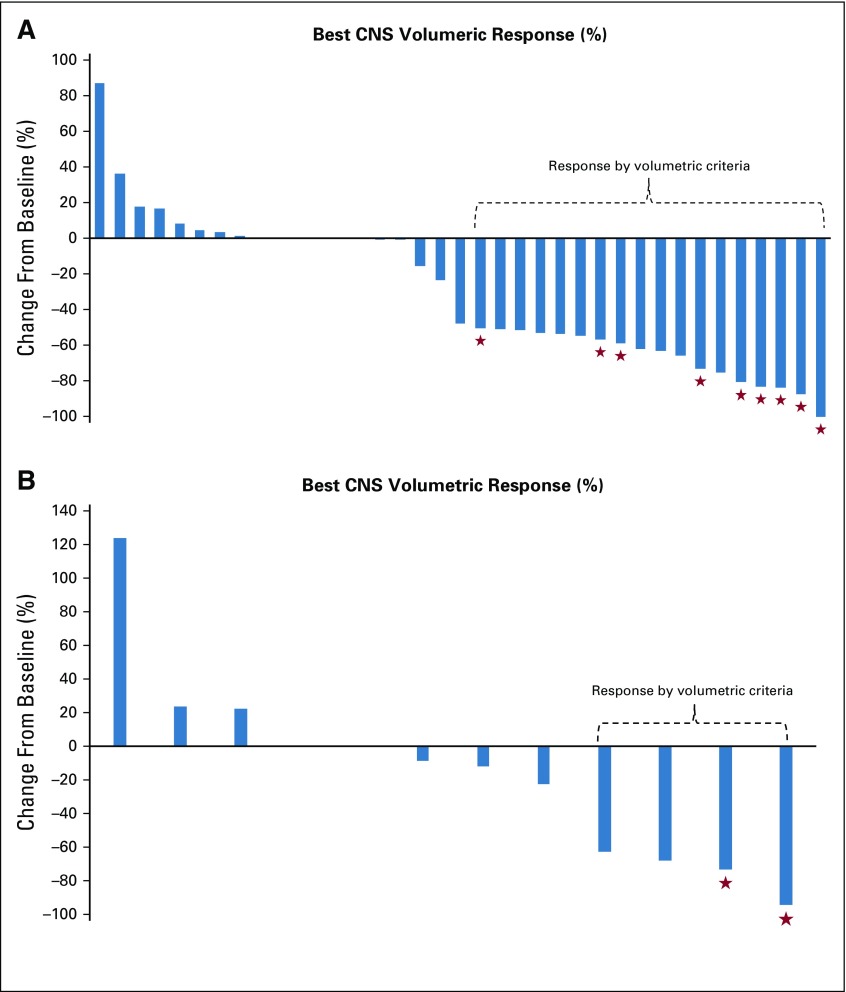
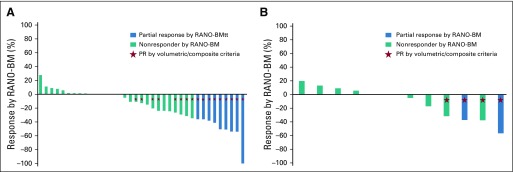
Patients and methods: Patients with measurable, progressive, HER2-positive brain metastases (92% after receiving CNS surgery and/or radiotherapy) received neratinib 240 mg orally once per day plus capecitabine 750 mg/m2 twice per day for 14 days, then 7 days off. Lapatinib-naïve (cohort 3A) and lapatinib-treated (cohort 3B) patients were enrolled. If nine or more of 35 (cohort 3A) or three or more of 25 (cohort 3B) had CNS objective response rates (ORR), the drug combination would be deemed promising. The primary end point was composite CNS ORR in each cohort separately, requiring a reduction of 50% or more in the sum of target CNS lesion volumes without progression of nontarget lesions, new lesions, escalating steroids, progressive neurologic signs or symptoms, or non-CNS progression.
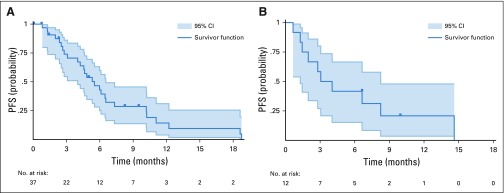
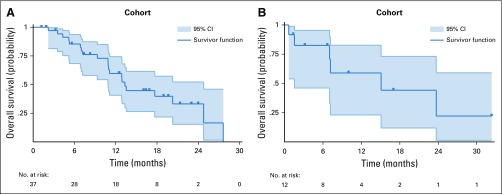
Results: Forty-nine patients enrolled in cohorts 3A (n = 37) and 3B (n = 12; cohort closed for slow accrual). In cohort 3A, the composite CNS ORR = 49% (95% CI, 32% to 66%), and the CNS ORR in cohort 3B = 33% (95% CI, 10% to 65%). Median progression-free survival was 5.5 and 3.1 months in cohorts 3A and 3B, respectively; median survival was 13.3 and 15.1 months. Diarrhea was the most common grade 3 toxicity (29% in cohorts 3A and 3B).
Neratinib plus capecitabine is active against refractory, HER2-positive breast cancer brain metastases, adding additional evidence that the efficacy of HER2-directed therapy in the brain is enhanced by chemotherapy. For optimal tolerance, efforts to minimize diarrhea are warranted.
Trial registration: ClinicalTrials.gov NCT01494662.
Figures
Comment in
-
Neratinib Plus Capecitabine Provides a Glimmer of Hope for a Daunting Disease.J Clin Oncol. 2019 May 1;37(13):1044-1046. doi: 10.1200/JCO.19.00083. Epub 2019 Mar 15. J Clin Oncol. 2019. PMID: 30875278 Free PMC article. No abstract available.
-
Brain metastases respond to neratinib plus capecitabine.Nat Rev Clin Oncol. 2019 Jun;16(6):336. doi: 10.1038/s41571-019-0207-3. Nat Rev Clin Oncol. 2019. PMID: 30940923 No abstract available.
References
-
- Lin NU, Winer EP. Brain metastases: The HER2 paradigm. Clin Cancer Res. 2007;13:1648–1655. - PubMed
-
- Bendell JC, Domchek SM, Burstein HJ, et al. Central nervous system metastases in women who receive trastuzumab-based therapy for metastatic breast carcinoma. Cancer. 2003;97:2972–2977. - PubMed
-
- Pestalozzi BC. Brain metastases and subtypes of breast cancer. Ann Oncol. 2009;20:803–805. - PubMed
-
- Kennecke H, Yerushalmi R, Woods R, et al. Metastatic behavior of breast cancer subtypes. J Clin Oncol. 2010;28:3271–3277. - PubMed
-
- Lin NU, Bellon JR, Winer EP. CNS metastases in breast cancer. J Clin Oncol. 2004;22:3608–3617. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
