

Predictive risk score for unplanned 30-day rehospitalizations in the French universal health care system based on a medico-administrative database
- PMID: 30861004
- PMCID: PMC6414180
- DOI: 10.1371/journal.pone.0210714
Predictive risk score for unplanned 30-day rehospitalizations in the French universal health care system based on a medico-administrative database
Abstract
Background: Reducing unplanned rehospitalizations is one of the priorities of health care policies in France and other Western countries. An easy-to-use algorithm for identifying patients at higher risk of rehospitalizations would help clinicians prioritize actions and care concerning discharge transitions. Our objective was to develop a predictive unplanned 30-day all-cause rehospitalization risk score based on the French hospital medico-administrative database.
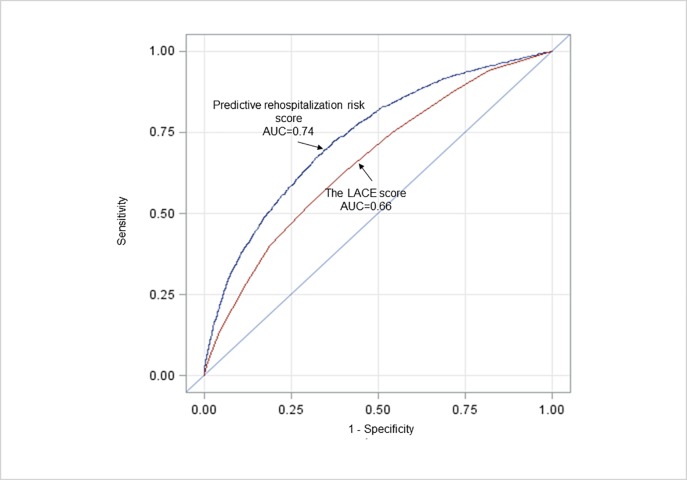
Methods: This was a retrospective cohort study of all 2015 discharges from acute-care inpatient hospitalizations in a tertiary-care university center comprising four hospitals. The study endpoint was unplanned 30-day all-cause rehospitalization via emergency departments, and we collected sociodemographic, clinical, and hospital characteristics based on hospitalization database computed for reimbursement of fees. We derived a predictive rehospitalization risk score using a split-sample design and multivariate logistic regression, and we compared the discriminative properties with the LACE index risk-score.
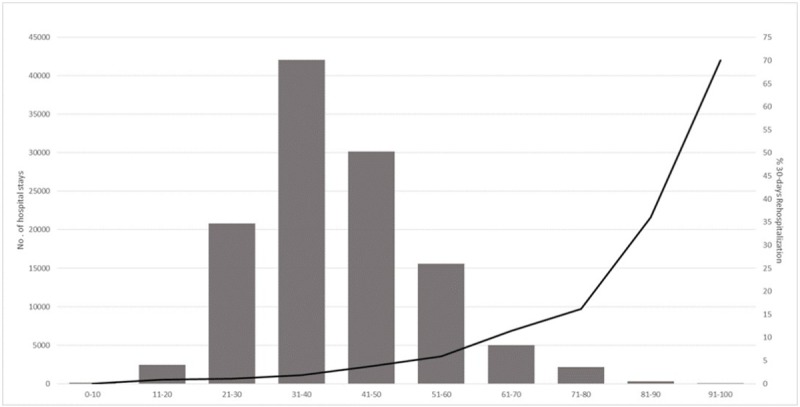
Result: Our analysis included 118,650 hospitalizations, of which 4,127 (3.5%) led to rehospitalizations via emergency departments. Variables independently associated with rehospitalization were age, gender, state-funded medical assistance, as well as disease category and severity, Charlson comorbidity index, hospitalization via emergency departments, length of stay (LOS), and previous hospitalizations 6 months before. The predictive rehospitalization risk score yielded satisfactory discriminant properties (C statistic: 0.74) exceeding the LACE index (0.66).
Conclusion: Our findings indicate that the possibility of unplanned rehospitalization remains high for some patient characteristics, indicating that targeted interventions could be beneficial for patients at the greatest risk. We developed an easy-to-use predictive rehospitalization risk-score of unplanned 30-day all-cause rehospitalizations with satisfactory discriminant properties. Future works should, however, explore if other data from electronic medical records and other databases could improve the accuracy of our predictive rehospitalization risk score based on medico-administrative data.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Machine-learning prediction of unplanned 30-day rehospitalization using the French hospital medico-administrative database.Medicine (Baltimore). 2020 Dec 4;99(49):e22361. doi: 10.1097/MD.0000000000022361. Medicine (Baltimore). 2020. PMID: 33285668 Free PMC article.
-
Multiyear Rehospitalization Rates and Hospital Outcomes in an Integrated Health Care System.JAMA Netw Open. 2019 Dec 2;2(12):e1916769. doi: 10.1001/jamanetworkopen.2019.16769. JAMA Netw Open. 2019. PMID: 31800072 Free PMC article.
-
Factors associated with unplanned readmissions in a major Australian health service.Aust Health Rev. 2019 Feb;43(1):1-9. doi: 10.1071/AH16287. Aust Health Rev. 2019. PMID: 29092726
-
Risk factors associated with paediatric unplanned hospital readmissions: a systematic review.BMJ Open. 2019 Jan 28;9(1):e020554. doi: 10.1136/bmjopen-2017-020554. BMJ Open. 2019. PMID: 30696664 Free PMC article.
-
Performance of French medico-administrative databases in epidemiology of infectious diseases: a scoping review.Front Public Health. 2023 May 12;11:1161550. doi: 10.3389/fpubh.2023.1161550. eCollection 2023. Front Public Health. 2023. PMID: 37250067 Free PMC article.
Cited by
-
Machine-learning prediction of unplanned 30-day rehospitalization using the French hospital medico-administrative database.Medicine (Baltimore). 2020 Dec 4;99(49):e22361. doi: 10.1097/MD.0000000000022361. Medicine (Baltimore). 2020. PMID: 33285668 Free PMC article.
-
Comparison of Back-Propagation Neural Network, LACE Index and HOSPITAL Score in Predicting All-Cause Risk of 30-Day Readmission.Risk Manag Healthc Policy. 2021 Sep 14;14:3853-3864. doi: 10.2147/RMHP.S318806. eCollection 2021. Risk Manag Healthc Policy. 2021. PMID: 34548831 Free PMC article.
-
Current Trends in Readmission Prediction: An Overview of Approaches.Arab J Sci Eng. 2021 Aug 16:1-18. doi: 10.1007/s13369-021-06040-5. Online ahead of print. Arab J Sci Eng. 2021. PMID: 34422543 Free PMC article.
-
Factors associated with early 14-day unplanned hospital readmission: a matched case-control study.BMC Health Serv Res. 2021 Aug 25;21(1):870. doi: 10.1186/s12913-021-06902-6. BMC Health Serv Res. 2021. PMID: 34433448 Free PMC article.
References
-
- Boutwell AE, Johnson MB, Rutherford P, Watson SR, Vecchioni N, Auerbach BS, et al. An early look at a four-state initiative to reduce avoidable hospital readmissions. Health Aff Proj Hope. 2011. July;30(7):1272–80. - PubMed
-
- HAS- Haute Autorité de Santé. Note méthodologique et de synthèse documentaire «Sortie d’hospitalisation supérieure à 24 heures–Établissement d’une check-list». In. Available from: http://www.has-sante.fr/portail/upload/docs/application/pdf/2015-05/note...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
