

Feasibility of lung cancer prediction from low-dose CT scan and smoking factors using causal models
- PMID: 30862725
- PMCID: PMC6585306
- DOI: 10.1136/thoraxjnl-2018-212638
Feasibility of lung cancer prediction from low-dose CT scan and smoking factors using causal models
Abstract
Introduction: Low-dose CT (LDCT) is currently used in lung cancer screening of high-risk populations for early lung cancer diagnosis. However, 96% of individuals with detected nodules are false positives.
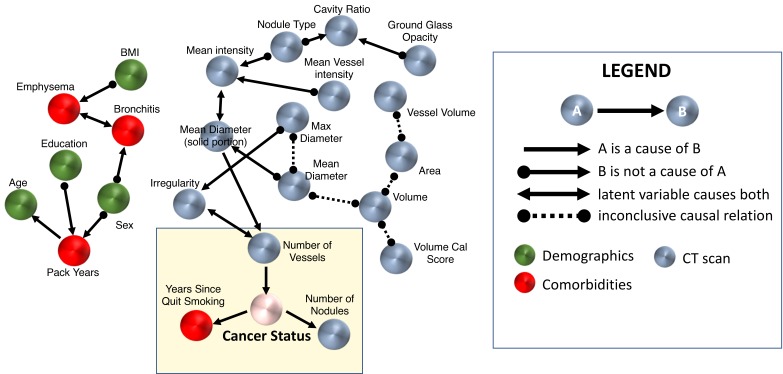
Methods: In order to develop an efficient early lung cancer predictor from clinical, demographic and LDCT features, we studied a total of 218 subjects with lung cancer or benign nodules. Probabilistic graphical models (PGMs) were used to integrate demographics, clinical data and LDCT features from 92 subjects (training cohort) from the Pittsburgh Lung Screening Study cohort.
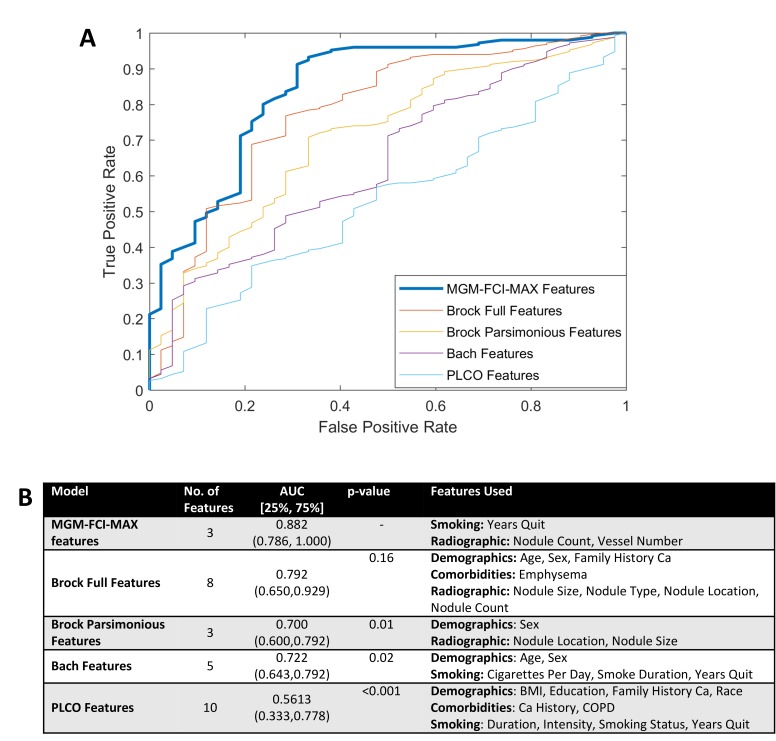
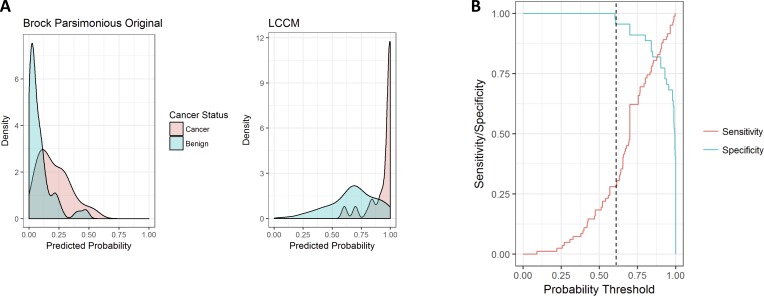
Results: Learnt PGMs identified three variables directly (causally) linked to malignant nodules and the largest benign nodule and used them to build the Lung Cancer Causal Model (LCCM), which was validated in a separate cohort of 126 subjects. Nodule and vessel numbers and years since the subject quit smoking were sufficient to discriminate malignant from benign nodules. Comparison with existing predictors in the training and validation cohorts showed that (1) incorporating LDCT scan features greatly enhances predictive accuracy; and (2) LCCM improves cancer detection over existing methods, including the Brock parsimonious model (p<0.001). Notably, the number of surrounding vessels, a feature not previously used in predictive models, significantly improves predictive efficiency. Based on the validation cohort results, LCCM is able to identify 30% of the benign nodules without risk of misclassifying cancer nodules.
Discussion: LCCM shows promise as a lung cancer predictor as it is significantly improved over existing models. Validated in a larger, prospective study, it may help reduce unnecessary follow-up visits and procedures.
Keywords: cancer screening; low-dose CT; lung cancer risk.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical