

NACT+IMRT versus NACT+IMRT+CCRT in locoregionally advanced NPC patients: a retrospective study
- PMID: 30863119
- PMCID: PMC6390870
- DOI: 10.2147/OTT.S183483
NACT+IMRT versus NACT+IMRT+CCRT in locoregionally advanced NPC patients: a retrospective study
Abstract
Purpose: The outcomes and safety profiles of neoadjuvant chemotherapy (NACT) + intensity modulated radiotherapy (IMRT) or NACT + IMRT + concurrent chemoradiotherapy (CCRT) in locoregionally advanced nasopharyngeal carcinoma (NPC) patients were retrospectively analyzed.
Patients and methods: Between 2010 and 2014, 125 patients with stage III-IVb NPC, who were treated with IMRT (36, 28.8%) or IMRT + CCRT (89, 71.2%) following NACT, participated in the research. There were grade 3-4 toxicities during NACT or radiotherapy (RT) in NACT + IMRT group and NACT + IMRT + CCRT group.
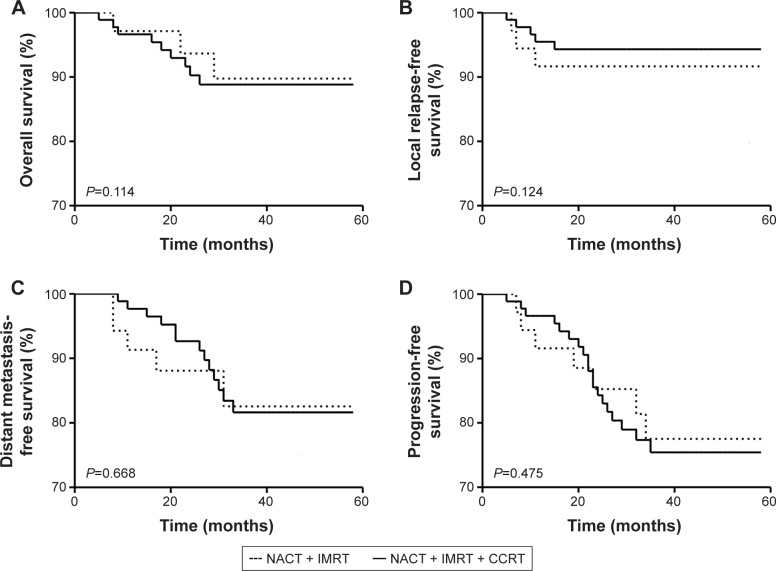
Results: MRI within 3 months demonstrated that no patient suffered with progressive disease, 116 patients (92.8%) achieved a response rate (RR) with the complete response (CR) rate of 70.4% (88/125) and partial response (PR) rate of 22.4% (28/125), and nine patients (7.2%) showed stable disease (SD) at the primary site and metastatic nodes. Compared with NACT + IMRT group, patients in NACT + IMRT + CCRT group did not show significantly better RR (93.3% vs 91.7%, P=1.00), CR rate (71.9% vs 66.7%, P=0.67), or PR rate (21.4% vs 25%, P=0.81). There was no significant difference in overall survival (OS, P=0.114), local relapse-free survival (LRFS, P=0.124), distant metastasis-free survival (DMFS, P=0.668) or progression-free survival (PFS, P=0.475) between NACT + IMRT group and NACT + IMRT + CCRT group. T classification (P=0.042) and N classification (P=0.021) were independent prognostic factors for DMFS.
Conclusion: To sum up, no significant difference was observed in combined RR, CR rate, LRFS, DMFS, PFS, or OS between the two groups.
Keywords: advanced nasopharyngeal carcinoma; concurrent chemoradiotherapy; intensity modulated radiotherapy; neoadjuvant chemotherapy.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Neoadjuvant chemotherapy plus intensity-modulated radiotherapy versus neoadjuvant chemotherapy plus concurrent chemoradiotherapy for ascending or descending types of nasopharyngeal carcinoma: A retrospective study.Am J Otolaryngol. 2022 Jan-Feb;43(1):103193. doi: 10.1016/j.amjoto.2021.103193. Epub 2021 Sep 3. Am J Otolaryngol. 2022. PMID: 34509080
-
Neoadjuvant chemotherapy followed by concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: A phase III multicentre randomised controlled trial.Eur J Cancer. 2017 Apr;75:14-23. doi: 10.1016/j.ejca.2016.12.039. Epub 2017 Feb 16. Eur J Cancer. 2017. PMID: 28214653 Clinical Trial.
-
Neoadjuvant chemotherapy plus intensity-modulated radiotherapy versus concurrent chemoradiotherapy plus adjuvant chemotherapy for the treatment of locoregionally advanced nasopharyngeal carcinoma: a retrospective controlled study.Chin J Cancer. 2016 Jan 6;35:2. doi: 10.1186/s40880-015-0076-9. Chin J Cancer. 2016. PMID: 26739148 Free PMC article.
-
Sequential induction chemotherapy plus intensity-modulated radiotherapy versus concurrent chemoradiotherapy in locoregionally advanced nasopharyngeal carcinoma: the three-year report of a phase II, single center, randomized, non-inferiority trial.Cancer Med. 2021 Jun;10(12):3886-3895. doi: 10.1002/cam4.3936. Epub 2021 May 6. Cancer Med. 2021. PMID: 33955190 Free PMC article. Clinical Trial.
-
A Systematic Review and Meta-Analysis of Studies Comparing Concurrent Chemoradiotherapy With Radiotherapy Alone in the Treatment of Stage II Nasopharyngeal Carcinoma.Front Oncol. 2022 Jul 12;12:843675. doi: 10.3389/fonc.2022.843675. eCollection 2022. Front Oncol. 2022. PMID: 35903695 Free PMC article.
Cited by
-
Individualised cumulative cisplatin dose for locoregionally advanced nasopharyngeal carcinoma patients based on induction chemotherapy response and tumour volume.Ther Adv Med Oncol. 2024 Oct 9;16:17588359241286222. doi: 10.1177/17588359241286222. eCollection 2024. Ther Adv Med Oncol. 2024. PMID: 39483137 Free PMC article.
-
Effect of COVID-19 Epidemic on Delay of Diagnosis and Treatment Path for Patients with Nasopharyngeal Carcinoma.Cancer Manag Res. 2020 May 25;12:3859-3864. doi: 10.2147/CMAR.S254093. eCollection 2020. Cancer Manag Res. 2020. PMID: 32547222 Free PMC article.
-
Effect of intensity-modulated radiation therapy on sciatic nerve injury caused by echinococcosis.Neural Regen Res. 2021 Mar;16(3):580-586. doi: 10.4103/1673-5374.293153. Neural Regen Res. 2021. PMID: 32985491 Free PMC article.
References
-
- Vokes EE, Liebowitz DN, Weichselbaum RR. Nasopharyngeal carcinoma. Lancet. 1997;350(9084):1087–1091. - PubMed
-
- Chan AT, Leung SF, Ngan RK, et al. Overall survival after concurrent cisplatin-radiotherapy compared with radiotherapy alone in locoregionally advanced nasopharyngeal carcinoma. J Natl Cancer Inst. 2005;97(7):536–539. - PubMed
-
- Al-Sarraf M, LeBlanc M, Giri PG, et al. Chemoradiotherapy versus radiotherapy in patients with advanced nasopharyngeal cancer: phase III randomized Intergroup study 0099. J Clin Oncol. 1998;16(4):1310–1317. - PubMed
-
- Langendijk JA, Leemans CR, Buter J, Berkhof J, Slotman BJ. The additional value of chemotherapy to radiotherapy in locally advanced nasopharyngeal carcinoma: a meta-analysis of the published literature. J Clin Oncol. 2004;22(22):4604–4612. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
