

Health care utilization and costs following amplified versus non-amplified molecular probe testing for symptomatic patients with suspected vulvovaginitis: a US commercial payer population
- PMID: 30863131
- PMCID: PMC6388970
- DOI: 10.2147/CEOR.S191831
Health care utilization and costs following amplified versus non-amplified molecular probe testing for symptomatic patients with suspected vulvovaginitis: a US commercial payer population
Abstract
Background: Vulvovaginitis (VV) is a common reason women seek medical attention in the USA. Both the non-specific clinical presentation and risk of preterm labor or delivery necessitate accurate identification of the causative agents to guide appropriate therapy. The diagnostic accuracy of amplified molecular probe testing (AMP) has been shown to exceed that of non-amplified molecular probe (NAMP) by 20%-25%.
Objective: To evaluate the impact of diagnosis with AMP testing on health care utilization, direct costs, and health outcomes, compared with NAMP, for symptomatic patients with suspected VV from a commercial payer perspective.
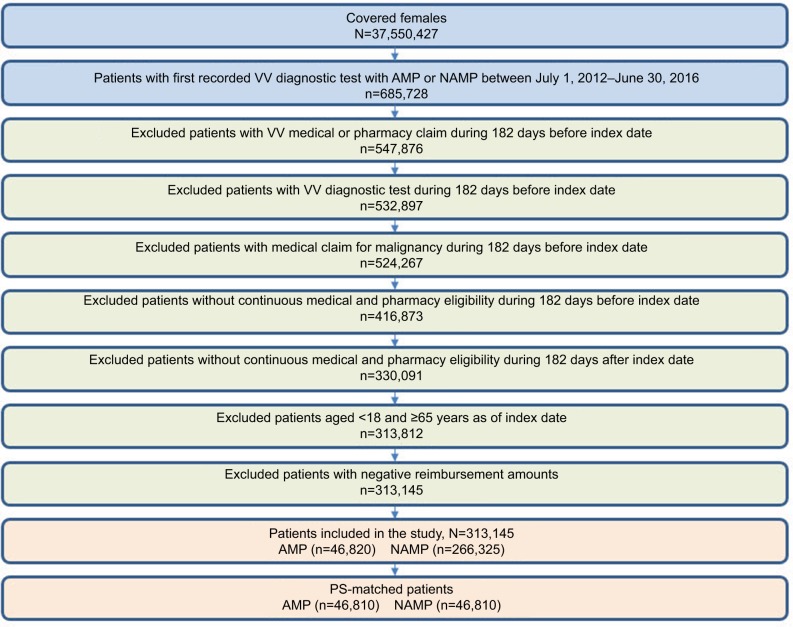
Methods: Symptomatic women (aged 18-64 years) who underwent VV testing with AMP or NAMP from January 1, 2012-December 31, 2016 were identified using the Truven Health Analytics MarketScan Database; those with continuous medical and pharmacy benefit enrollment 6 months pre/post AMP or NAMP testing were included. Patients were propensity score (PS) matched and 6-month all-cause health care resource utilization, all-cause direct costs (2017 USD), risk of all-cause hospitalization, and risk of preterm labor or delivery were compared between cohorts.
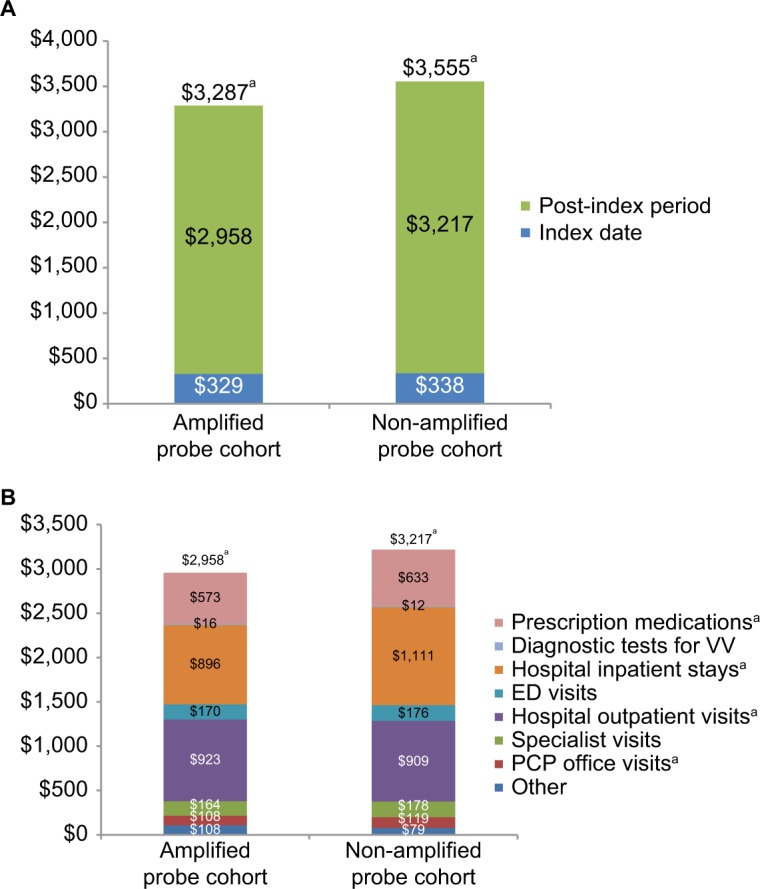
Results: After PS match (N=46,810 per group, mean age 34.2 years), AMP had significantly (all P<0.0001) fewer mean hospital outpatient visits (AMP 0.9 vs NAMP 1.0), primary care physician office visits (AMP 1.1 vs NAMP 1.2), and prescription medications (AMP 7.3 vs NAMP 8.0), and a 21% reduction in risk of hospitalization (risk ratio [RR]=0.79, 95% CI= 0.75-0.83, P<0.0001). Total medical expenditures per patient were lower for AMP than NAMP (mean AMP $3,287 vs NAMP $3,555, P<0.0001). Among pregnant women (N=2,175 per group), AMP had a 12% reduction in risk of preterm labor or delivery (RR =0.88, 95% CI=0.77-0.99, P=0.041).
Conclusion: This real-world study offers evidence on the clinical utility for symptomatic patients with suspected VV diagnosed with AMP compared to NAMP - demonstrating an opportunity to improve the patient journey while delivering value-based care.
Keywords: NuSwab; amplified molecular probe testing; clinical utility; costs; health care utilization; preterm delivery; preterm labor; propensity-score matching; vulvovaginitis.
Conflict of interest statement
Disclosure At the time of this study, Dr Ackerman, Mr Knight, and Dr Wahl were employed by Covance Inc., which is wholly owned by LabCorp, and Dr Cartwright was employed by LabCorp. Dr Ackerman and Mr Knight are shareholders in LabCorp. Dr Cartwright is an inventor on issued patents (9,057,111; 9,624,552; 9,970,064) relevant to this work and is a shareholder in LabCorp. The authors report no other conflicts of interest in this work.
Figures
References
-
- Kent HL. Epidemiology of vaginitis. Am J Obstet Gynecol. 1991;165(4 Pt 2):1168–1176. - PubMed
-
- van der Pol B. Diagnosing vaginal infections: it’s time to join the 21st century. Curr Infect Dis Rep. 2010;12(3):225–230. - PubMed
-
- Granato PA. Vaginitis: clinical and laboratory aspects for diagnosis. Clin Microbiol Newsl. 2010;32(15):111–116.
-
- Sobel JD. Vaginal infections in adult women. Med Clin North Am. 1990;74(6):1573–1602. - PubMed
LinkOut - more resources
Full Text Sources
