

Preoperative aspartate aminotransferase-to-platelet-ratio index as a predictor of posthepatectomy liver failure for resectable hepatocellular carcinoma
- PMID: 30863151
- PMCID: PMC6388945
- DOI: 10.2147/CMAR.S186114
Preoperative aspartate aminotransferase-to-platelet-ratio index as a predictor of posthepatectomy liver failure for resectable hepatocellular carcinoma
Abstract
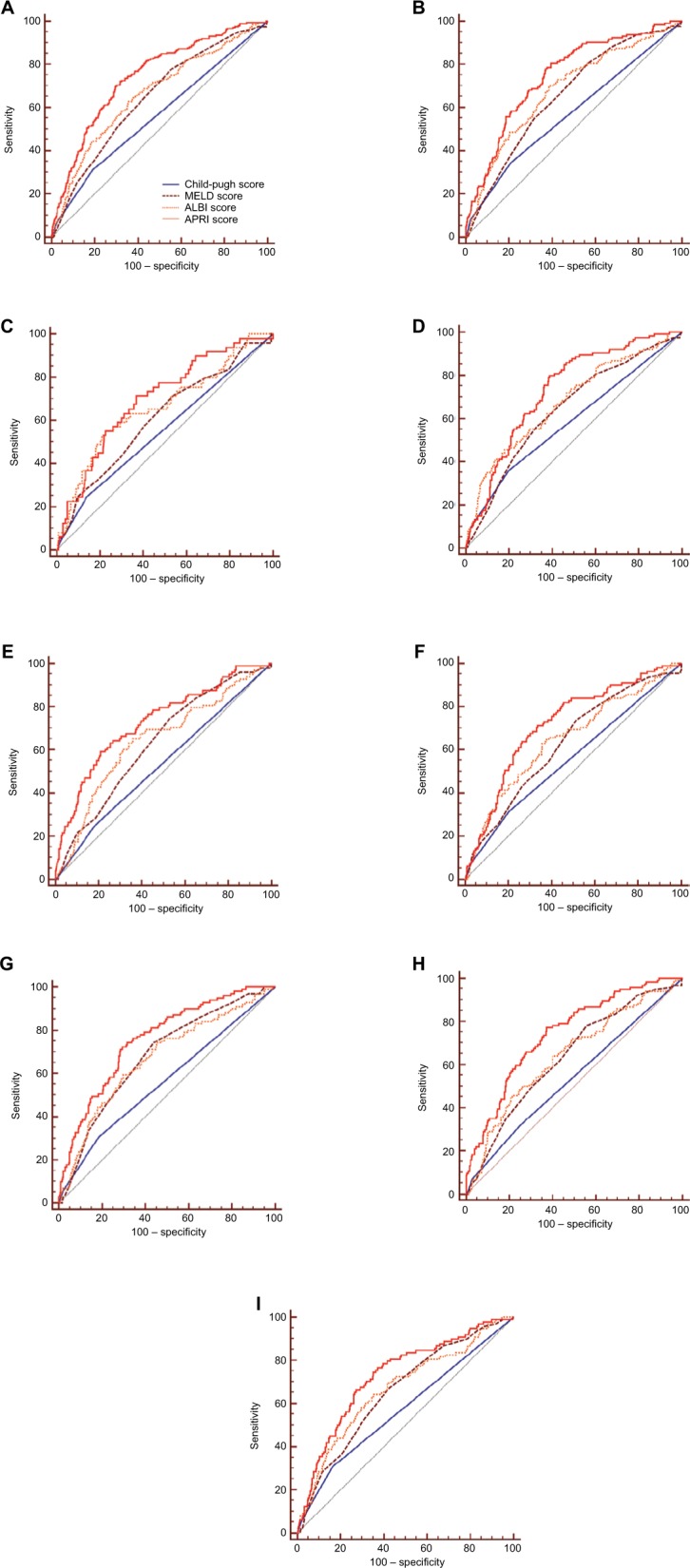
Purpose: This study aimed to investigate the efficacy of preoperative aspartate aminotransferase-to-platelet-ratio index (APRI) score to predict the risk of posthepatectomy liver failure (PHLF) in patients with hepatocellular carcinoma (HCC) after liver resection, and to compare the discriminatory performance of the APRI with the Child-Pugh score, model for end-stage liver disease (MELD) score, and albumin-bilirubin (ALBI) score.
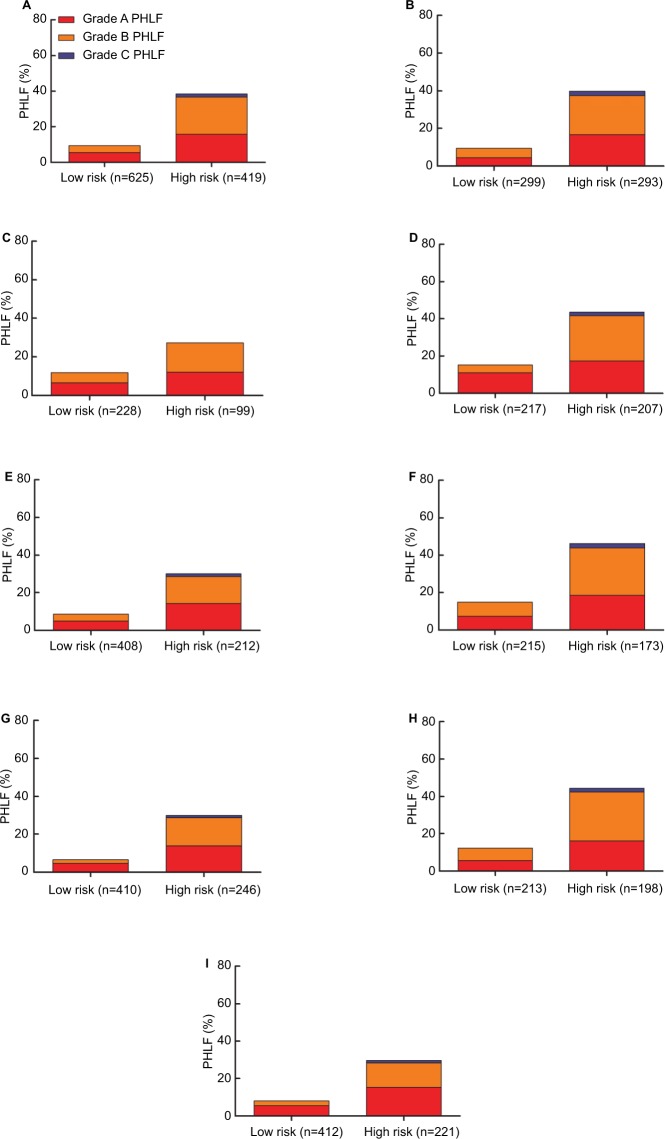
Patients and methods: A total of 1,044 consecutive patients with HCC who underwent liver resection were enrolled and studied. Univariate and multivariate analyses were performed to investigate risk factors associated with PHLF. Predictive discrimination of Child-Pugh, MELD, ALBI, and APRI scores for predicting PHLF were assessed according to area under the ROC curve. The cutoff value of the APRI score for predicting PHLF was determined by ROC analysis. APRI scores were stratified by dichotomy to analyze correlations with incidence and grade of PHLF.
Results: PHLF occurred in 213 (20.4%) patients. Univariate and multivariate analyses revealed that Child-Pugh, MELD, ALBI, and APRI scores were significantly associated with PHLF. Area under the ROC analysis revealed that the APRI score for predicting PHLF was significantly more accurate than Child-Pugh, MELD, or ALBI scores. With an optimal cutoff value of 0.55, the sensitivity and specificity of the APRI score for predicting PHLF were 72.2% and 68.0%, respectively, and the incidence and grade of PHLF in patients with high risk (APRI score >0.55) was significantly higher than in the low-risk cohort (APRI score <0.55).
Conclusion: The APRI score predicted PHLF in patients with HCC undergoing liver resection more accurately than Child-Pugh, MELD, or ALBI scores.
Keywords: Child–Pugh score; albumin-bilirubin score; aspartate aminotransferase-to-platelet ratio index; hepatocellular carcinoma; liver resection; model for end-stage liver disease score; posthepatectomy liver failure.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin. 2017;67(1):7–30. - PubMed
-
- Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380. - PubMed
-
- European Association for the Study of the Liver Electronic address: easloffice@easloffice.eu; European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. - PubMed
-
- Zhong JH, Ke Y, Gong WF, et al. Hepatic resection associated with good survival for selected patients with intermediate and advanced-stage hepatocellular carcinoma. Ann Surg. 2014;260(2):329–340. - PubMed
LinkOut - more resources
Full Text Sources
