

Addition of Cervical Elastography May Increase Preterm Delivery Prediction Performance in Pregnant Women with Short Cervix: a Prospective Study
- PMID: 30863266
- PMCID: PMC6406042
- DOI: 10.3346/jkms.2019.34.e68
Addition of Cervical Elastography May Increase Preterm Delivery Prediction Performance in Pregnant Women with Short Cervix: a Prospective Study
Abstract
Background: We investigated whether there is a difference in elastographic parameters between pregnancies with and without spontaneous preterm delivery (sPTD) in women with a short cervix (≤ 25 mm), and examined the ability of elastographic parameters to predict sPTD in those women.
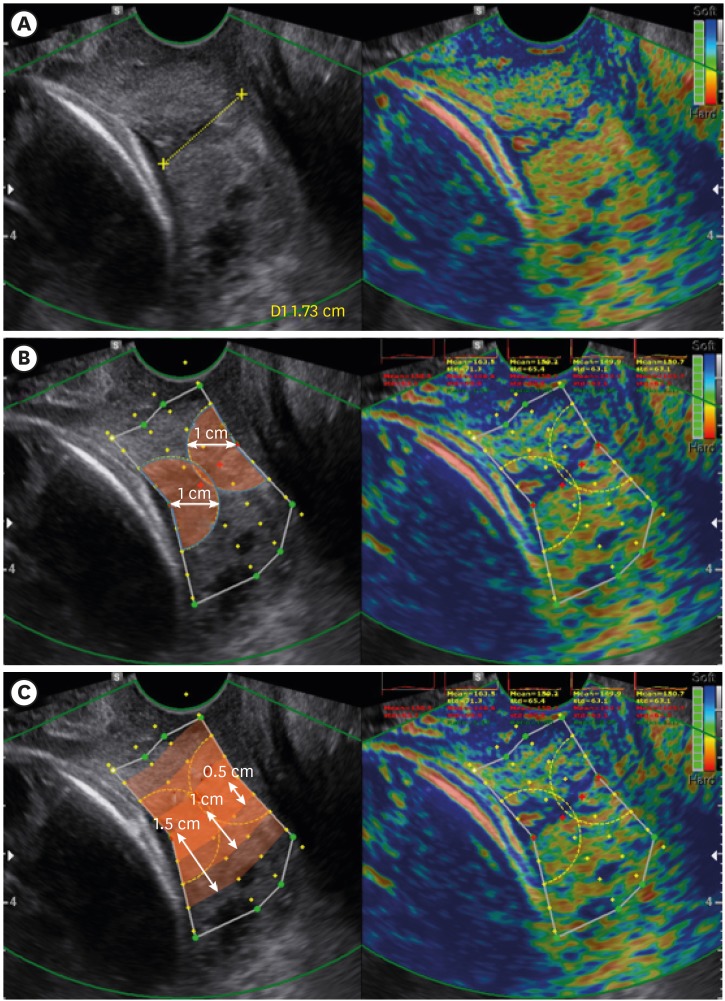
Methods: E-CervixTM (WS80A; Samsung Medison, Seoul, Korea) elastography was used to examine the cervical strain. Elastographic parameters were compared between pregnancies with and without sPTD. Diagnostic performance of elastographic parameters to predict sPTD ≤ 37 weeks, both alone and in combination with other parameters, was compared with that of cervical length (CL) using area under receiver operating characteristic curve (AUC) analysis.
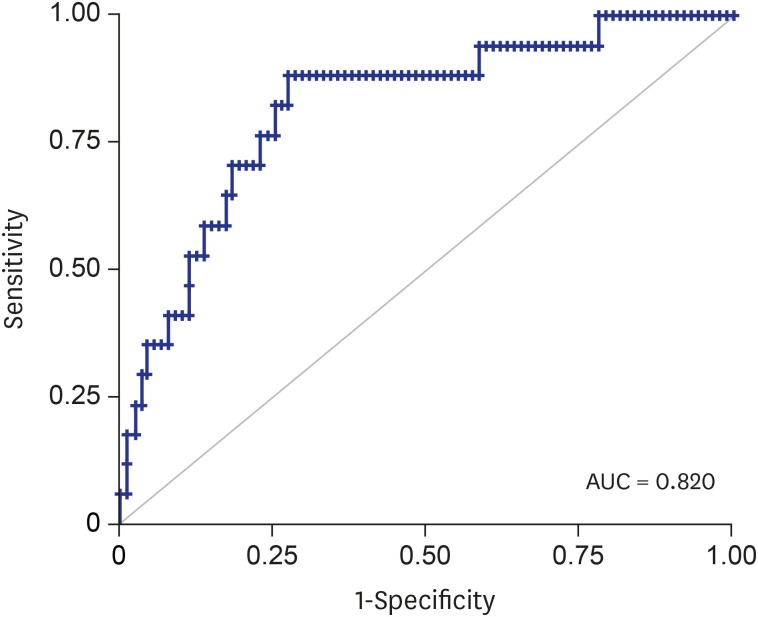
Results: A total of 130 women were included. Median gestational age (GA) at examination was 24.4 weeks (interquartile range, 21.4-28.9), and the prevalence of sPTD was 20.0% (26/130). Both the elastographic parameters and CL did not show statistical difference between those with and without sPTD. However, when only patients with CL ≥ 1.5 cm (n = 110) were included in the analysis, there was a significant difference between two groups in elasticity contrast index (ECI) within 0.5/1.0/1.5 cm from the cervical canal (P < 0.05) which is one of elastographic parameters generated by E-Cervix. When AUC analysis was performed in women with CL ≥ 1.5 cm, the combination of parameters (CL + pre-pregnancy body mass index + GA at exam + ECI within 0.5/1.0/1.5 cm) showed a significantly higher AUC than CL alone (P < 0.05).
Conclusion: An addition of cervical elastography may improve the ability to predict sPTD in women with a short CL between 1.5 and 2.5 cm.
Keywords: Elastography; Pregnancy; Preterm Delivery; Short Cervix; Strain; Ultrasonography.
Conflict of interest statement
Disclosure: The authors have no potential conflicts of interest to disclose.
Figures

Similar articles
-
The Feasibility of Cervical Elastography in Predicting Preterm Delivery in Singleton Pregnancy with Short Cervix Following Progesterone Treatment.Int J Environ Res Public Health. 2021 Feb 19;18(4):2026. doi: 10.3390/ijerph18042026. Int J Environ Res Public Health. 2021. PMID: 33669696 Free PMC article.
-
TVS-guided cervical strain elastography is more effective than measuring cervical length as an independent predictor of spontaneous preterm delivery in asymptomatic, high-risk women during the mid-trimester.J Matern Fetal Neonatal Med. 2024 Dec;37(1):2381589. doi: 10.1080/14767058.2024.2381589. Epub 2024 Jul 25. J Matern Fetal Neonatal Med. 2024. PMID: 39054066
-
Cervical elastography in predicting spontaneous preterm birth in singleton pregnancy with a short cervix receiving progesterone treatment at 18 to 24 weeks' gestation.J Matern Fetal Neonatal Med. 2024 Dec;37(1):2347954. doi: 10.1080/14767058.2024.2347954. Epub 2024 May 7. J Matern Fetal Neonatal Med. 2024. PMID: 38714523
-
Diagnostic accuracy of cervical elastography in predicting preterm delivery: A systematic review and meta-analysis.Medicine (Baltimore). 2019 Jul;98(29):e16449. doi: 10.1097/MD.0000000000016449. Medicine (Baltimore). 2019. PMID: 31335700 Free PMC article.
-
The effect of gestational age and cervical length measurements in the prediction of spontaneous preterm birth in twin pregnancies: an individual patient level meta-analysis.BJOG. 2016 May;123(6):877-84. doi: 10.1111/1471-0528.13575. Epub 2015 Sep 1. BJOG. 2016. PMID: 26333191 Review.
Cited by
-
The Feasibility of Cervical Elastography in Predicting Preterm Delivery in Singleton Pregnancy with Short Cervix Following Progesterone Treatment.Int J Environ Res Public Health. 2021 Feb 19;18(4):2026. doi: 10.3390/ijerph18042026. Int J Environ Res Public Health. 2021. PMID: 33669696 Free PMC article.
-
Nomogram Incorporating Multimodal Transvaginal Ultrasound Assessment at 20 to 24 Weeks' Gestation for Predicting Spontaneous Preterm Delivery in Low-Risk Women.Int J Womens Health. 2022 Mar 3;14:323-331. doi: 10.2147/IJWH.S356167. eCollection 2022. Int J Womens Health. 2022. PMID: 35264886 Free PMC article.
-
Repeatability and reproducibility of quantitative cervical strain elastography (E-Cervix) in pregnancy.Sci Rep. 2021 Dec 8;11(1):23689. doi: 10.1038/s41598-021-02498-3. Sci Rep. 2021. PMID: 34880263 Free PMC article.
-
Midtrimester cervical elastography in pregnant women with a history of loop electrosurgical excision procedure (LEEP).Sci Rep. 2022 Jun 2;12(1):9191. doi: 10.1038/s41598-022-13170-9. Sci Rep. 2022. PMID: 35655076 Free PMC article.
-
Prediction model for successful induction of labor by cervical strain elastography diagnosed at late-term pregnancy in nulliparous women: a prospective cohort study.BMC Pregnancy Childbirth. 2023 Feb 14;23(1):114. doi: 10.1186/s12884-023-05426-7. BMC Pregnancy Childbirth. 2023. PMID: 36788485 Free PMC article.
References
-
- Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, Narwal R, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379(9832):2162–2172. - PubMed
-
- Iams JD, Goldenberg RL, Meis PJ, Mercer BM, Moawad A, Das A, et al. The length of the cervix and the risk of spontaneous premature delivery. National Institute of Child Health and Human Development Maternal Fetal Medicine Unit Network. N Engl J Med. 1996;334(9):567–572. - PubMed
-
- Berghella V, Palacio M, Ness A, Alfirevic Z, Nicolaides KH, Saccone G. Cervical length screening for prevention of preterm birth in singleton pregnancy with threatened preterm labor: systematic review and meta-analysis of randomized controlled trials using individual patient-level data. Ultrasound Obstet Gynecol. 2017;49(3):322–329. - PubMed
