

Safety of an improved patent ductus arteriosus occluder for transcatheter closure of perimembranous ventricular septal defects with abnormally attached tricuspid chordae tendineae
- PMID: 30863756
- PMCID: PMC6406192
- DOI: 10.12998/wjcc.v7.i5.562
Safety of an improved patent ductus arteriosus occluder for transcatheter closure of perimembranous ventricular septal defects with abnormally attached tricuspid chordae tendineae
Abstract
Background: The off-label use of various devices has been reported for the transcatheter closure of perimembranous ventricular septal defects (PmVSD) because of serious complications, such as heart block and tricuspid regurgitation (TR), associated with conventional ventricular septal defect devices. However, whether certain defects such as PmVSD with abnormally attached tricuspid are fit for interventional treatment is still disputable.
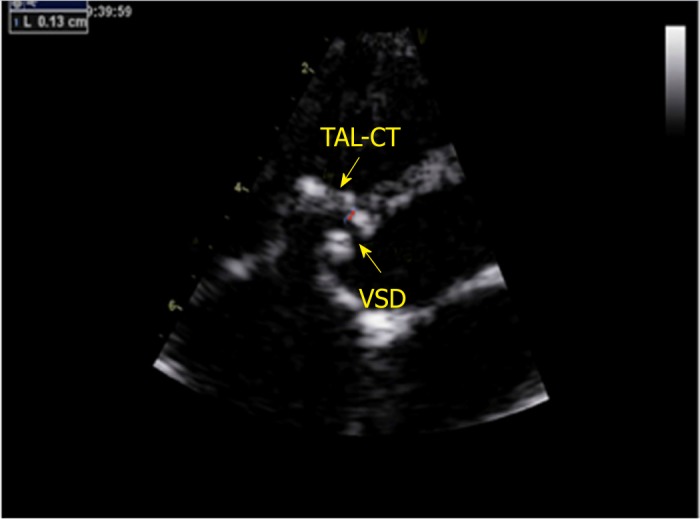
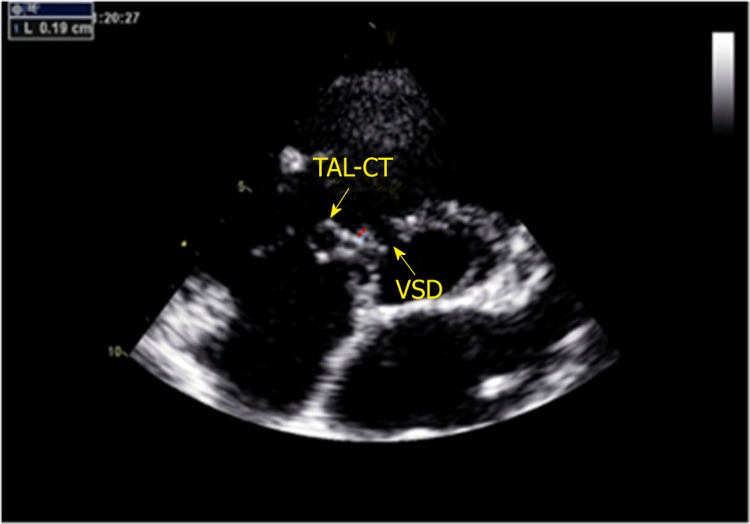
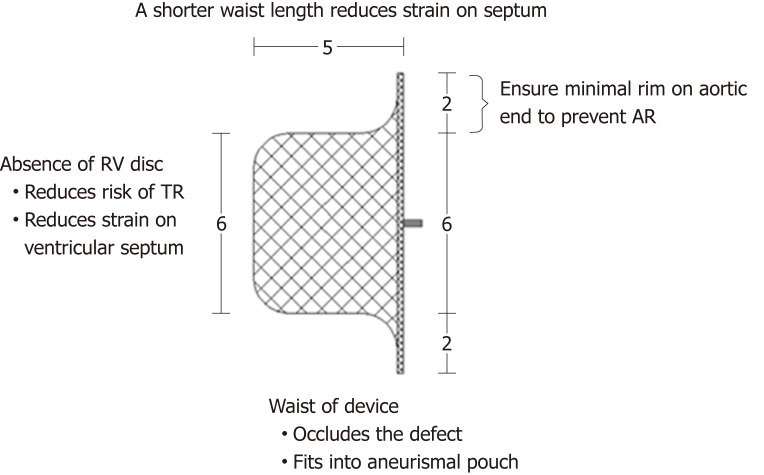
Aim: To explore the feasibility and safety of transcatheter closure of PmVSD with abnormally attached tricuspid chordae tendineae using an improved patent ductus arteriosus (PDA) occluder.
Methods: We retrospectively analyzed 20 patients diagnosed with PmVSD with abnormally attached tricuspid chordae tendineae who underwent interventional treatment using an improved PDA occluder at our center from January 2012 to January 2016. Baseline characteristics and procedural and follow-up data were analyzed.
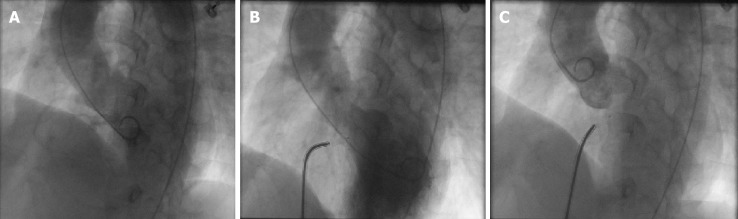
Results: All 20 patients achieved procedure success. No heart block occurred during the operation. One patient had a transient complete right bundle branch block within 48 h post-procedure and reverted to normal rhythm after intravenous injections of dexamethasone for 3 d. For all 20 patients, no residual shunt was observed by transthoracic echocardiography post-procedure. During the average follow-up period of 2.4 years, no severe TR was observed.
Conclusion: Using of the improved PDA occluder for the transcatheter closure of PmVSD with abnormally attached tricuspid chordae tendineae is a safe and promising treatment option. However, long-term follow-up in a large group of patients is still warranted.
Keywords: Chordae tendineae; Patent ductus arteriosus occlude; Transcatheter; Tricuspid regurgitation; Ventricular septal defect.
Conflict of interest statement
Conflict-of-interest statement: None.
Figures
Similar articles
-
Transcatheter closure of perimembranous ventricular septal defect using Amplatzer ductal occluder.Catheter Cardiovasc Interv. 2013 Dec 1;82(7):1141-6. doi: 10.1002/ccd.24810. Epub 2013 Aug 20. Catheter Cardiovasc Interv. 2013. PMID: 23554093
-
[Complications of transcatheter interventional occlusion of ventricular septal defects].Zhonghua Er Ke Za Zhi. 2005 Jan;43(1):35-8. Zhonghua Er Ke Za Zhi. 2005. PMID: 15796806 Chinese.
-
Midterm Results of Transaxillary Occluder Device Closure of Perimembranous Ventricular Septal Defect Guided Solely by Transesophageal Echocardiography.Heart Surg Forum. 2019 Mar 8;22(2):E112-E118. doi: 10.1532/hsf.2185. Heart Surg Forum. 2019. PMID: 31013220
-
Transcatheter closure of perimembranous and intracristal ventricular septal defects with the SHSMA occluder.Catheter Cardiovasc Interv. 2012 Mar 1;79(4):666-74. doi: 10.1002/ccd.23344. Epub 2011 Dec 8. Catheter Cardiovasc Interv. 2012. PMID: 22109986
-
[Efficacy of the transcatheter closure of perimembranous and muscular ventricular septal defects with the Amplatzer duct occluder II].Zhonghua Xin Xue Guan Bing Za Zhi. 2012 Oct;40(10):817-20. Zhonghua Xin Xue Guan Bing Za Zhi. 2012. PMID: 23302666 Chinese.
References
-
- Wei Y, Wang X, Zhang S, Hou L, Wang Y, Xu Y, Sun Q, Zhao H. Transcatheter closure of perimembranous ventricular septal defects (VSD) with VSD occluder: early and mid-term results. Heart Vessels. 2012;27:398–404. - PubMed
-
- Pedra CA, Pedra SR, Esteves CA, Pontes SC, Jr, Braga SL, Arrieta SR, Santana MV, Fontes VF, Masura J. Percutaneous closure of perimembranous ventricular septal defects with the Amplatzer device: technical and morphological considerations. Catheter Cardiovasc Interv. 2004;61:403–410. - PubMed
-
- Butera G, Carminati M, Chessa M, Piazza L, Micheletti A, Negura DG, Abella R, Giamberti A, Frigiola A. Transcatheter closure of perimembranous ventricular septal defects: early and long-term results. J Am Coll Cardiol. 2007;50:1189–1195. - PubMed
-
- Carminati M, Butera G, Chessa M, De Giovanni J, Fisher G, Gewillig M, Peuster M, Piechaud JF, Santoro G, Sievert H, Spadoni I, Walsh K Investigators of the European VSD Registry. Transcatheter closure of congenital ventricular septal defects: results of the European Registry. Eur Heart J. 2007;28:2361–2368. - PubMed
LinkOut - more resources
Full Text Sources
