

Sero-Prevalence Surveillance to Predict Vaccine-Preventable Disease Outbreaks; A Lesson from the 2014 Measles Epidemic in Northern Vietnam
- PMID: 30863786
- PMCID: PMC6405937
- DOI: 10.1093/ofid/ofz030
Sero-Prevalence Surveillance to Predict Vaccine-Preventable Disease Outbreaks; A Lesson from the 2014 Measles Epidemic in Northern Vietnam
Abstract
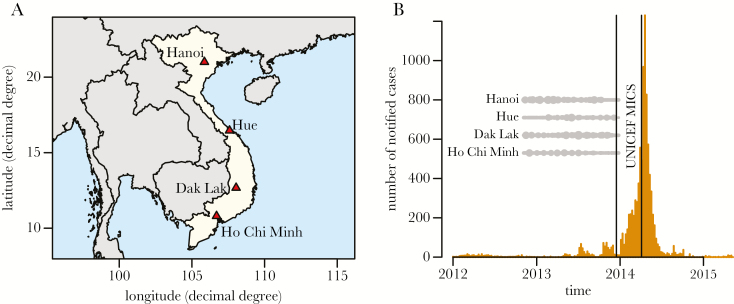
Background: During the first half of 2014, a severe outbreak of measles occurred in northern Vietnam, causing 15 033 confirmed cases and 146 deaths.
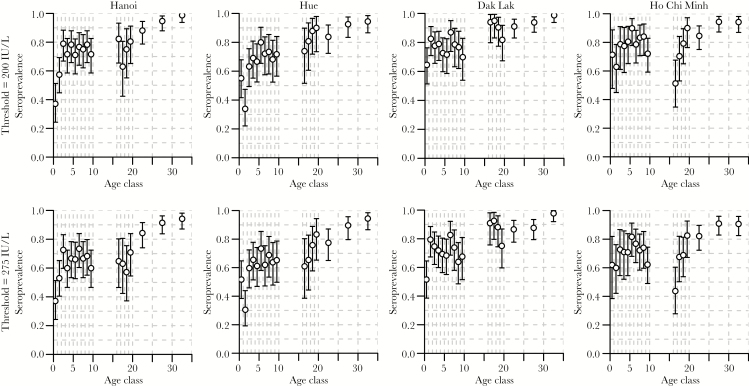
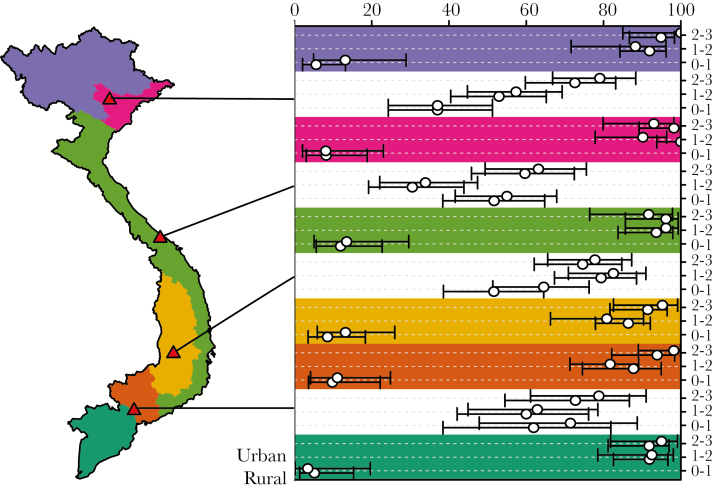
Methods: To evaluate the population-level seroprevalence of protection against measles in the period before the outbreak, we made use of an existing age-stratified serum bank, collected over the year before the outbreak, between November 2012 and December 2013, from 4 sites across the country (Hanoi, Hue, Dak Lak, and Ho Chi Minh City). Data from the UNICEF's Multiple Indicator Clustered Surveys (MICS), carried out in Vietnam during the first quarter of 2014, were used to assess the vaccine coverage in 6 ecological regions of Vietnam.
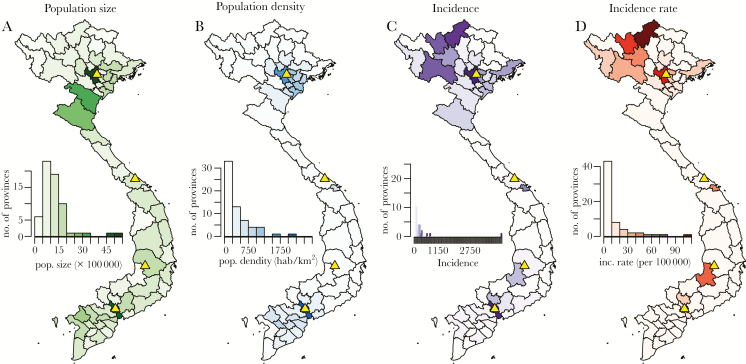
Results: Results revealed a large discrepancy between levels of protection, as estimated from the serology and vaccine coverage estimated by UNICEF's MICS. Variation in seroprevalence across locations and age groups corresponded with reported numbers of measles cases, most of which were among the 0-2-year-old age group and in the northern part of the country.
Conclusions: Our study presents a strong case in favor of a serosurveillance sentinel network that could be used to proactively tune vaccination policies and other public health interventions.
Keywords: Vietnam; measles; seroprevalence; vaccination.
Figures
References
-
- Perry RT, Halsey NA. The clinical significance of measles: a review. J Infect Dis 2004; 189(Suppl 1):S4–16. - PubMed
-
- Strebel P, Cochi S, Grabowsky M, et al. The unfinished measles immunization agenda. J Infect Dis 2003; 187(Suppl 1):S1–7. - PubMed
-
- Cliff AD, Haggett P, Smallman-Raynor M.. Measles: An Historical Geography of a Major Human Viral Disease from Global Expansion to Local Retreat, 1840–1990. Oxford, UK: Blackwell; 1993.
-
- van den Ent MMVX, Brown DW, Hoekstra EJ, et al. Measles mortality reduction contributes substantially to reduction of all cause mortality among children less than five years of age, 1990–2008. J Infect Dis 2011; 204(Suppl 1):S18–23. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
