

Liver resection versus transarterial chemoembolization for the treatment of intermediate-stage hepatocellular carcinoma
- PMID: 30864247
- PMCID: PMC6488138
- DOI: 10.1002/cam4.2038
Liver resection versus transarterial chemoembolization for the treatment of intermediate-stage hepatocellular carcinoma
Abstract
Background: The role of transarterial chemoembolization (TACE) as the standard treatment for intermediate-stage hepatocellular carcinoma (HCC) is being challenged by increasing studies supporting liver resection (LR); but evidence of survival benefits of LR is lacking. We aimed to compare the overall survival (OS) of LR with that of TACE for the treatment of intermediate-stage HCC in cirrhotic patients.
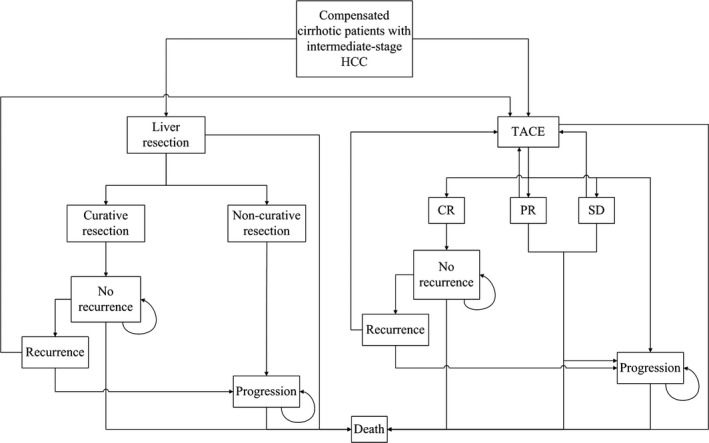
Methods: A Markov model, comparing LR with TACE over 15 years, was developed based on the data from 31 literatures. Additionally, external validation of the model was performed using a data set (n = 1735; LR: 701; TACE: 1034) from a tertiary center with propensity score matching method. We conducted one-way and two-way sensitivity analyses, in addition to a Monte Carlo analysis with 10 000 patients allocated into each arm.
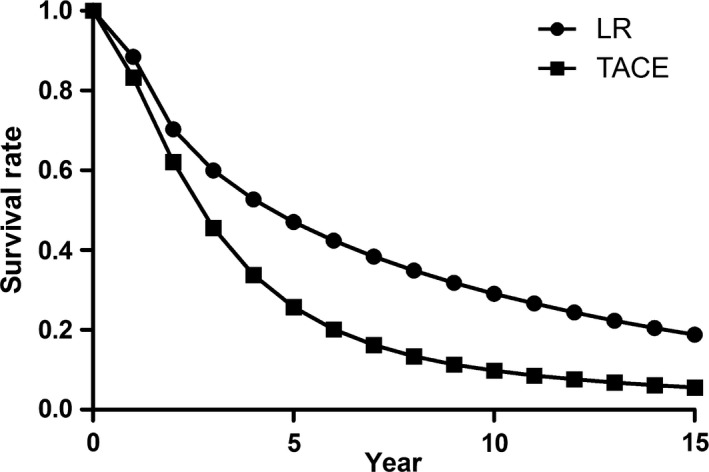
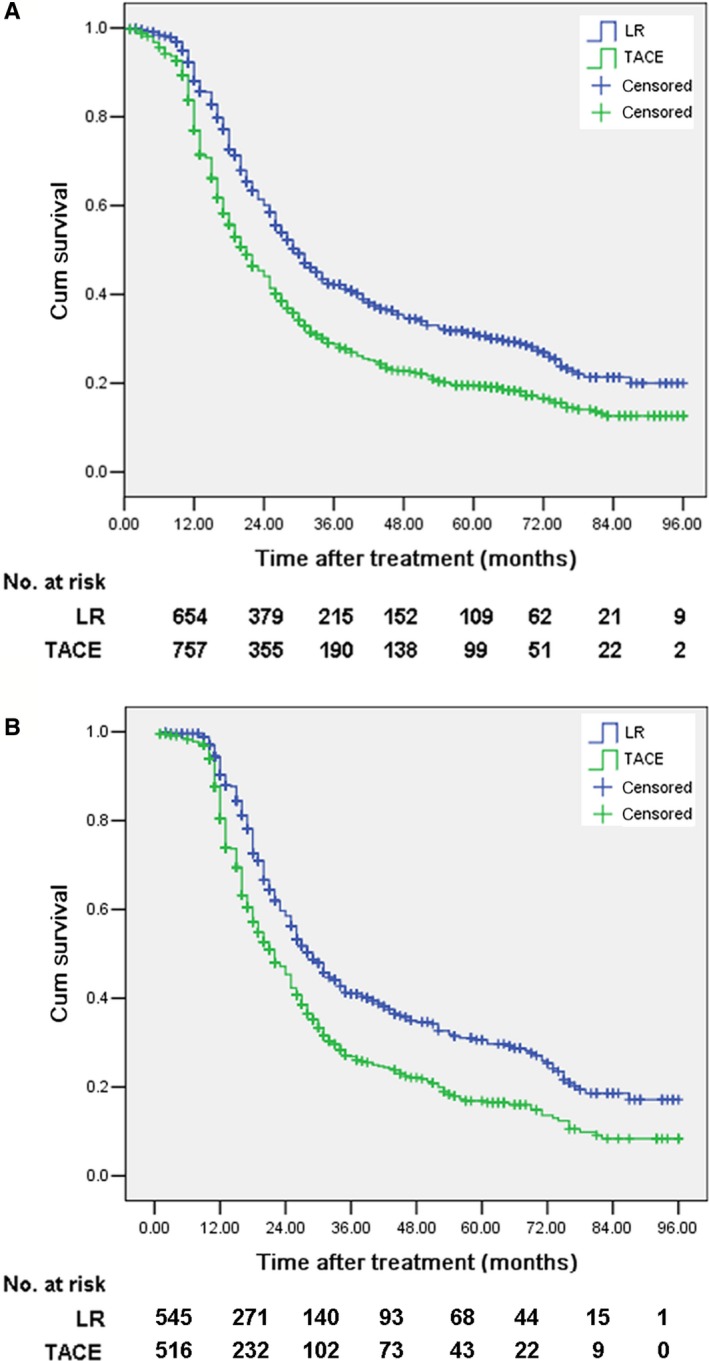
Results: The mean expected survival times and survival rates at 5 years were 77.8 months and 47.1% in LR group, and 48.6 months and 25.7% in TACE group, respectively. Sensitivity analyses found that initial LR was the most favorable treatment. The 95% CI for the difference in OS was 2.42-2.46 years between the two groups (P < 0.001). In the validation set, the 5-year survival rates after LR were significantly better than those after TACE before (40.2% vs. 25.9%, P < 0.001) and after matching (43.2% vs 30.9%, P < 0.001), which was comparable to the model results.
Conclusions: For cirrhotic patients with resectable intermediate-stage HCC, LR may provide survival benefit over TACE, but large-scale studies are required to further stratify patients at this stage for different optimal treatments.
Keywords: Markov Model; intermediate-stage hepatocellular carcinoma; liver resection; propensity score matching; transarterial chemoembolization.
© 2019 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
All coauthors have seen and agreed with the content of the manuscript and there is no financial interest to report.
Figures
Similar articles
-
Comparison of hepatic resection and transarterial chemoembolization for UICC stage T3 hepatocellular carcinoma: a propensity score matching study.BMC Cancer. 2018 Jun 7;18(1):643. doi: 10.1186/s12885-018-4557-5. BMC Cancer. 2018. PMID: 29879928 Free PMC article.
-
Comparison of overall survival on surgical resection versus transarterial chemoembolization with or without radiofrequency ablation in intermediate stage hepatocellular carcinoma: a propensity score matching analysis.BMC Gastroenterol. 2020 Apr 10;20(1):99. doi: 10.1186/s12876-020-01235-w. BMC Gastroenterol. 2020. PMID: 32272898 Free PMC article.
-
Liver resection versus transarterial chemoembolization for the initial treatment of Barcelona Clinic Liver Cancer stage B hepatocellular carcinoma.Hepatol Int. 2018 Sep;12(5):417-428. doi: 10.1007/s12072-018-9888-4. Epub 2018 Aug 2. Hepatol Int. 2018. PMID: 30073454
-
Comparison of transarterial chemoembolization with radiofrequency ablation for unresectable Barcelona Clinic Liver Cancer stage 0/A hepatocellular carcinoma: a propensity score matching.J Gastroenterol Hepatol. 2016 Feb;31(2):442-9. doi: 10.1111/jgh.13077. J Gastroenterol Hepatol. 2016. PMID: 26259976
-
Transarterial chemoembolization versus hepatic resection in hepatocellular carcinoma treatment: a meta-analysis.Drug Des Devel Ther. 2015 Aug 10;9:4431-40. doi: 10.2147/DDDT.S86629. eCollection 2015. Drug Des Devel Ther. 2015. PMID: 26309396 Free PMC article. Review.
Cited by
-
Tumor Burden Score and Serum Alpha-fetoprotein Subclassify Intermediate-Stage Hepatocellular Carcinoma.J Gastrointest Surg. 2022 Dec;26(12):2512-2521. doi: 10.1007/s11605-022-05469-9. Epub 2022 Sep 28. J Gastrointest Surg. 2022. PMID: 36171471
-
The priority of liver resection compared with transarterial chemoembolization in hepatocellular carcinoma at BCLC B1 stage: A single-center experience.Front Surg. 2022 Nov 9;9:920976. doi: 10.3389/fsurg.2022.920976. eCollection 2022. Front Surg. 2022. PMID: 36439533 Free PMC article.
-
Integrating the new systemic treatment landscape and surgical therapy in hepatocellular carcinoma.Turk J Surg. 2024 Mar 23;40(1):1-10. doi: 10.47717/turkjsurg.2024.6375. eCollection 2024 Mar. Turk J Surg. 2024. PMID: 39036000 Free PMC article. Review.
-
State-of-the-art surgery for hepatocellular carcinoma.Langenbecks Arch Surg. 2021 Nov;406(7):2151-2162. doi: 10.1007/s00423-021-02298-3. Epub 2021 Aug 18. Langenbecks Arch Surg. 2021. PMID: 34405284
-
Surgical resection for large hepatocellular carcinoma and those beyond BCLC: systematic review with proposed management algorithm.Langenbecks Arch Surg. 2023 Apr 12;408(1):144. doi: 10.1007/s00423-023-02881-w. Langenbecks Arch Surg. 2023. PMID: 37041364
References
-
- Forner A, Gilabert M, Bruix J, Raoul JL. Treatment of intermediate‐stage hepatocellular carcinoma. Nat Rev Clin Oncol. 2014;11:525‐535. - PubMed
-
- Llovet JM, Bruix J. Novel advancements in the management of hepatocellular carcinoma in 2008. J Hepatol. 2008;48(Suppl 1):S20‐S37. - PubMed
-
- Ho MC, Huang GT, Tsang YM, et al. Liver resection improves the survival of patients with multiple hepatocellular carcinomas. Ann Surg Oncol. 2009;16:848‐855. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
