

Evaluation of Drinking Risk Levels as Outcomes in Alcohol Pharmacotherapy Trials: A Secondary Analysis of 3 Randomized Clinical Trials
- PMID: 30865232
- PMCID: PMC6450273
- DOI: 10.1001/jamapsychiatry.2018.3079
Evaluation of Drinking Risk Levels as Outcomes in Alcohol Pharmacotherapy Trials: A Secondary Analysis of 3 Randomized Clinical Trials
Abstract
Importance: The US Food and Drug Administration recognizes total abstinence and no heavy drinking days as outcomes for pivotal pharmacotherapy trials for alcohol use disorder (AUD). Many patients have difficulty achieving these outcomes, which can discourage seeking treatment and has slowed the development of medications that affect alcohol use.
Objective: To compare 2 drinking-reduction outcomes with total abstinence and no heavy drinking outcomes.
Design, setting, and participants: Data were obtained from 3 multisite, randomized, placebo-controlled clinical trials of medications for treating alcohol dependence (naltrexone, varenicline, and topiramate) in adults with DSM-IV-categorized alcohol dependence.
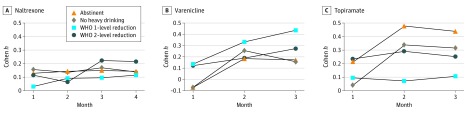
Main outcomes and measures: Within each trial, the percentage of participants in active and placebo conditions who met responder definitions of abstinence, no heavy drinking days, a WHO 1-level reduction, and a WHO 2-level reduction was computed by month with corresponding effect sizes (Cohen h).
Results: Across the 3 trials (N = 1169; mean [SD] age, 45 [10] years; 824 [70.5%] men), the percentage of participants classified as responders during the last 4 weeks of treatment was lowest for abstinence (naltrexone, 34.7% [100 of 288]; varenicline, 7.3% [7 of 96]; topiramate, 11.7% [21 of 179]) followed by no heavy drinking days (naltrexone, 51.0% [147 of 288]; varenicline, 24.0% [23 of 96]; topiramate, 20.7% [37 of 179]), WHO 2-level reduction (naltrexone, 75.0% [216 of 288]; varenicline, 55.2% [53 of 96]; topiramate, 44.7% [80 of 179]), and WHO 1-level reduction (naltrexone, 83.3% [240 of 288]; varenicline, 69.8 [67 of 96]; topiramate, 54.7% [98 of 179]) outcomes. Standardized treatment effects observed for the WHO 2-level reduction outcomes (naltrexone, Cohen h = 0.214 [95% CI, 0.053 -0.375]; varenicline, 0.273 [95% CI, -0.006 to 0.553]; topiramate, 0.230 [95% CI, 0.024-0.435]) and WHO 1-level reduction (naltrexone, Cohen h = 0.116 [95% CI, -0.046 to 0.277]; varenicline, 0.338 [95% CI, 0.058-0.617]; topiramate, 0.014 [95% CI, -0.192 to 0.219]) were comparable with those obtained using abstinence (naltrexone, Cohen h = 0.142 [95% CI, -0.020 to 0.303]; varenicline, 0.146 [95% CI, -0.133 to 0.426]; topiramate, 0.369 [95% CI, 0.163-0.574]) and no heavy drinking days (naltrexone, Cohen h = 0.140 [95% CI, -0.021 to 0.302]; varenicline, 0.232 [95% CI, -0.048 to 0.511]; topiramate, 0.207 [95% CI, 0.002-0.413]).
Conclusions and relevance: WHO drinking risk level reductions appear to be worthwhile indicators of treatment outcome in AUD pharmacotherapy trials. These outcomes may align with drinking reduction goals of many patients and capture clinically meaningful improvements experienced by more patients than either abstinence or no heavy drinking days.
Trial registration: ClinicalTrials.gov identifiers: NCT00006206; NCT01146613; NCT00210925.
Conflict of interest statement
Figures
Comment in
-
Why Less Is Always More in the Treatment of Alcohol Use Disorders.JAMA Psychiatry. 2019 Apr 1;76(4):359-360. doi: 10.1001/jamapsychiatry.2018.2807. JAMA Psychiatry. 2019. PMID: 30865234 No abstract available.
-
Weniger Alkoholkonsum dank Arzneimitteln.MMW Fortschr Med. 2019 Dec;161(21-22):32. doi: 10.1007/s15006-019-1226-9. MMW Fortschr Med. 2019. PMID: 31828641 German. No abstract available.
References
-
- Centers for Disease Control and Prevention (CDC) Alcohol and public health: alcohol-related disease impact application (ARDI): 2013. http://nccd.cdc.gov/DPH_ARDI/default/default.aspx. Accessed March 7, 2018.
-
- Grant BF, Chou SP, Saha TD, et al. . Prevalence of 12-month alcohol use, high-risk drinking, and DSM-IV alcohol use disorder in the United States, 2001-2002 to 2012-2013: results from the National Epidemiologic Survey on Alcohol and Related Conditions. JAMA Psychiatry. 2017;74(9):911-923. doi:10.1001/jamapsychiatry.2017.2161 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
