

Mutational Analysis of Patients With Colorectal Cancer in CALGB/SWOG 80405 Identifies New Roles of Microsatellite Instability and Tumor Mutational Burden for Patient Outcome
- PMID: 30865548
- PMCID: PMC6506418
- DOI: 10.1200/JCO.18.01798
Mutational Analysis of Patients With Colorectal Cancer in CALGB/SWOG 80405 Identifies New Roles of Microsatellite Instability and Tumor Mutational Burden for Patient Outcome
Abstract
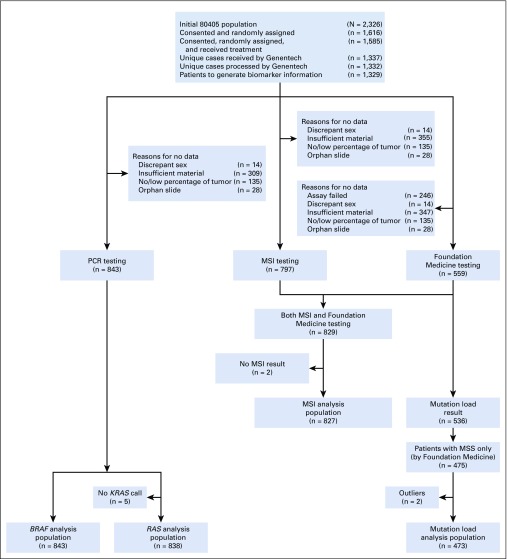
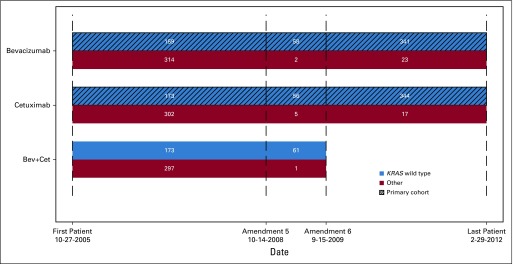
Purpose: CALGB/SWOG 80405 was a randomized phase III trial that found no statistically significant difference in overall survival (OS) in patients with first-line metastatic colorectal cancer treated with chemotherapy plus either bevacizumab or cetuximab. Primary tumor DNA from 843 patients has been used to discover genetic markers of OS.
Patients and methods: Gene mutations were determined by polymerase chain reaction. Microsatellite status was determined by genotyping of microsatellites. Tumor mutational burden (TMB) was determined by next-generation sequencing. Cox proportional hazard models were used, with adjusting factors. Interaction of molecular alterations with either the bevacizumab or the cetuximab arms was tested.
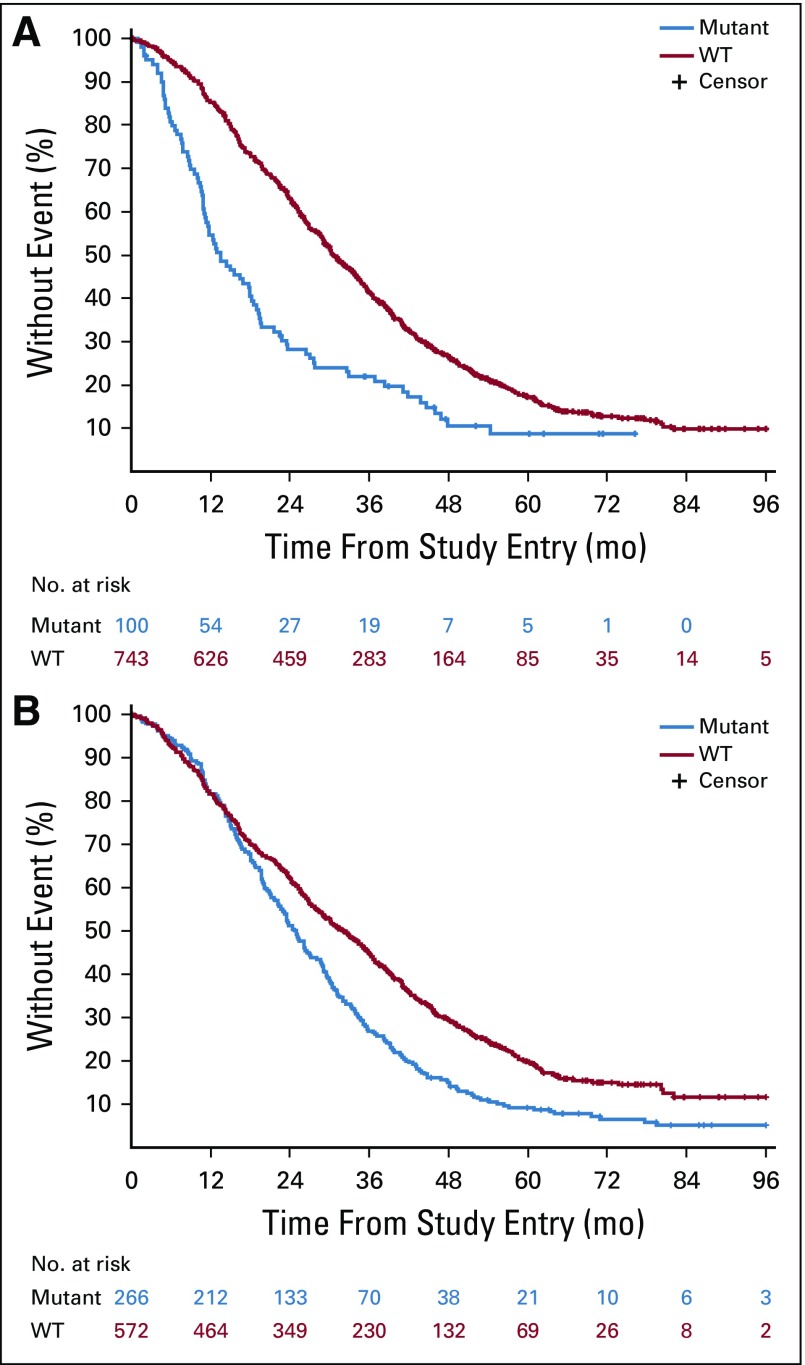
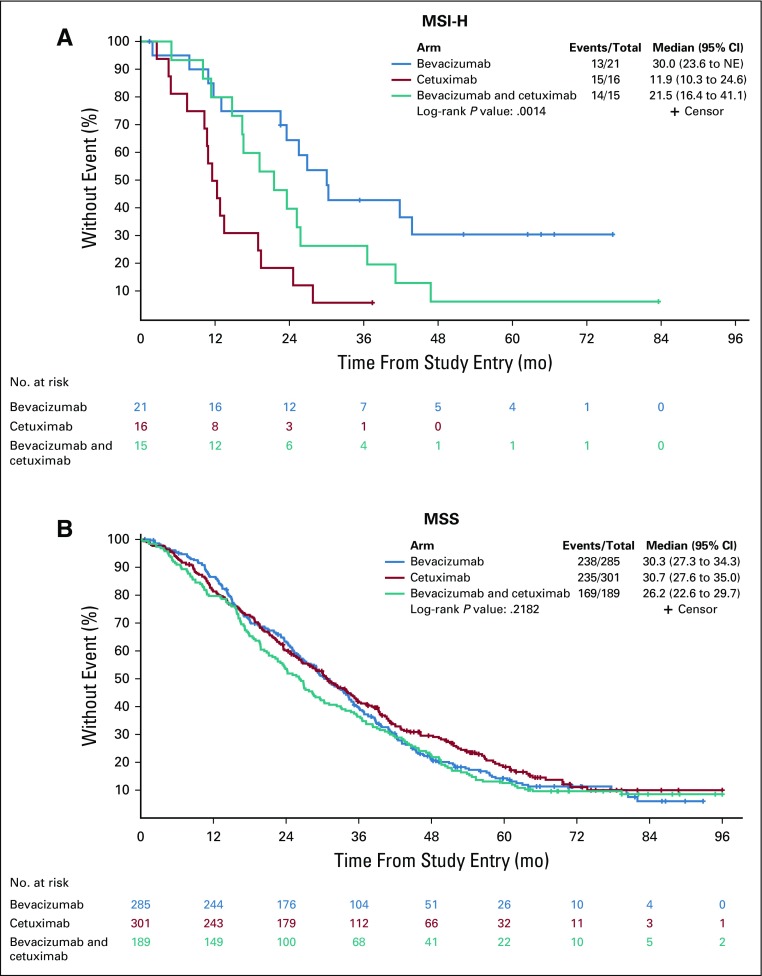
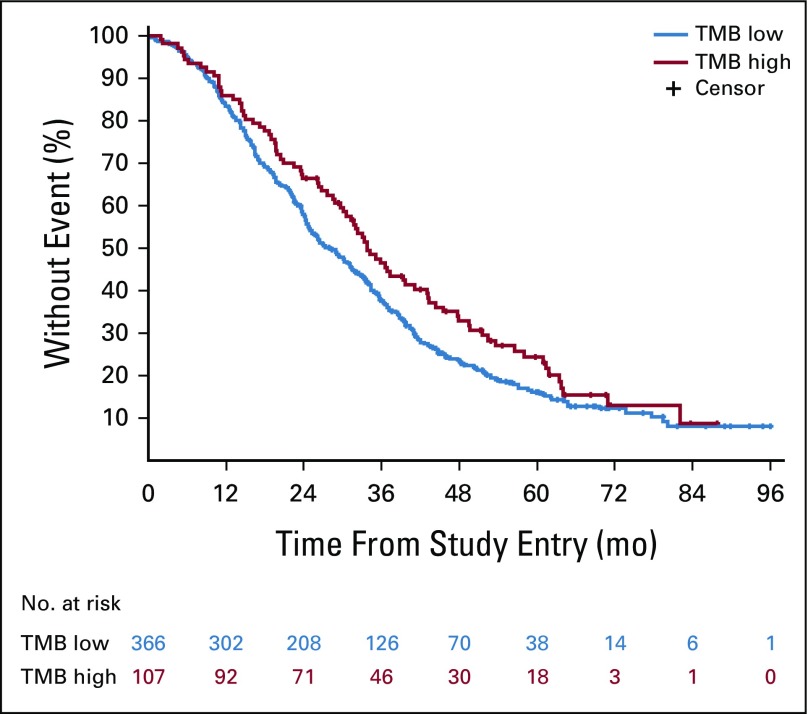
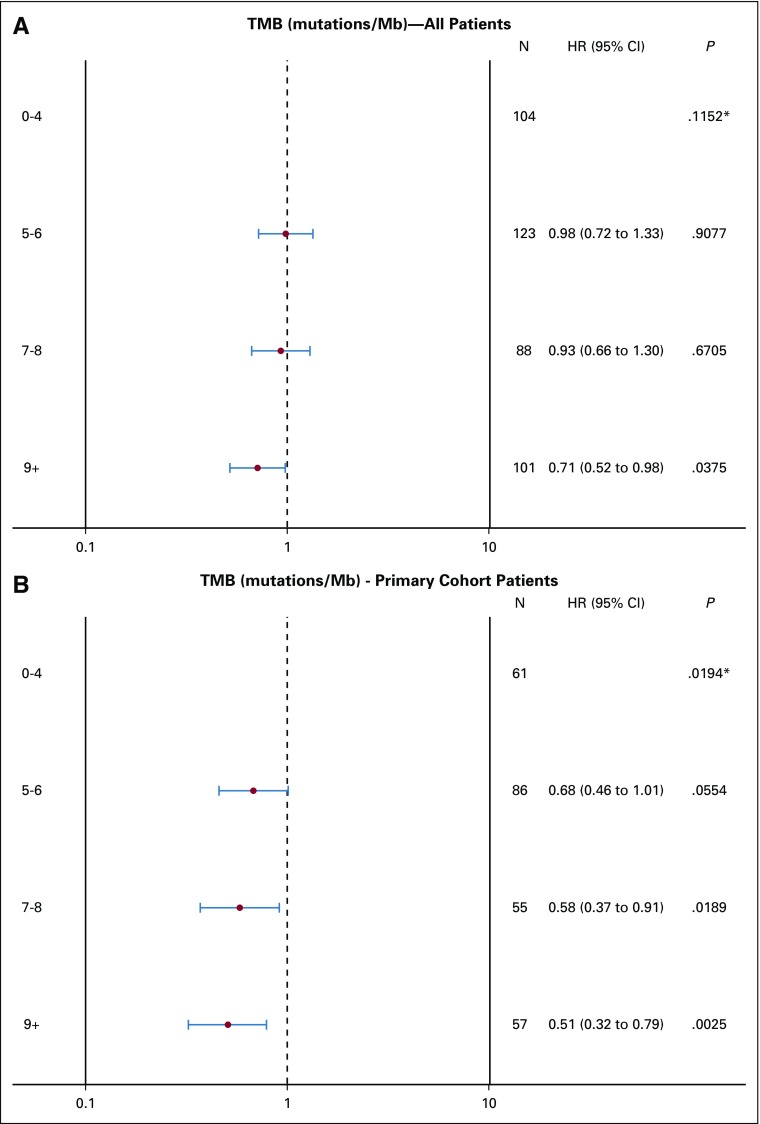
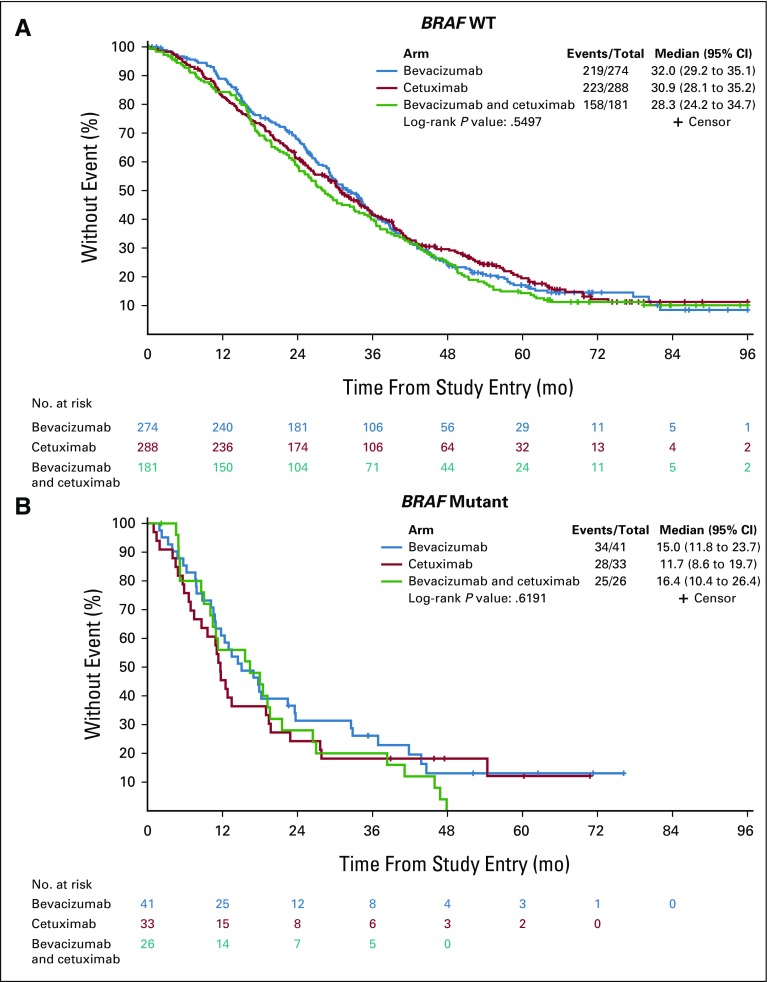
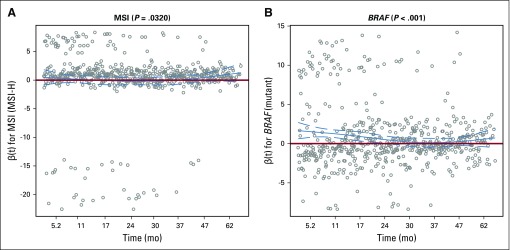
Results: Patients with high TMB in their tumors had longer OS than did patients with low TMB (hazard ratio [HR], 0.73 [95% CI, 0.57 to 0.95]; P = .02). In patients with microsatellite instability-high (MSI-H) tumors, longer OS was observed in the bevacizumab arm than in the cetuximab arm (HR, 0.13 [95% CI, 0.06 to 0.30]; interaction P < .001 for interaction between microsatellite status and the two arms). Patients with BRAF mutant tumors had shorter OS than did patients with wild-type (WT) tumors (HR, 2.01 [95% CI, 1.49 to 2.71]; P < .001). Patients with extended RAS mutant tumors had shorter OS than did patients with WT tumors (HR, 1.52 [95% CI, 1.26 to 1.84]; P < .001). Patients with triple-negative tumors (WT for NRAS/KRAS/BRAF) had a median OS of 35.9 months (95% CI, 33.0 to 38.8 months) versus 22.2 months (95% CI, 19.6 to 24.4 months ) in patients with at least one mutated gene in their tumors (P < .001).
Conclusion: In patients with metastatic colorectal cancer treated in first line, low TMB, and BRAF and RAS mutations are negative prognostic factors. Patients with MSI-H tumors benefited more from bevacizumab than from cetuximab, and studies to confirm this effect of MSI-H are warranted.
Figures

Comment in
-
TMB is linked with prognosis.Nat Rev Clin Oncol. 2019 Jun;16(6):336. doi: 10.1038/s41571-019-0206-4. Nat Rev Clin Oncol. 2019. PMID: 30932077 No abstract available.
-
Molecular Markers of Molecular Markers.J Clin Oncol. 2019 Sep 1;37(25):2291. doi: 10.1200/JCO.19.00746. Epub 2019 Jul 3. J Clin Oncol. 2019. PMID: 31268797 No abstract available.
-
Reply to S. Sorscher.J Clin Oncol. 2019 Sep 1;37(25):2291-2293. doi: 10.1200/JCO.19.01366. Epub 2019 Jul 3. J Clin Oncol. 2019. PMID: 31268798 No abstract available.
References
-
- Siegel RL, Miller KD, Fedewa SA, et al. Colorectal cancer statistics, 2017. CA Cancer J Clin. 2017;67:177–193. - PubMed
-
- Contal C, O’Quigley J. An application of changepoint methods in studying the effect of age on survival in breast cancer. Comput Stat Data Anal. 1999;30:253–270.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
