

Reducing High-Dose Opioid Prescribing: State-Level Morphine Equivalent Daily Dose Policies, 2007-2017
- PMID: 30865779
- PMCID: PMC8607298
- DOI: 10.1093/pm/pnz038
Reducing High-Dose Opioid Prescribing: State-Level Morphine Equivalent Daily Dose Policies, 2007-2017
Abstract
Objective: To describe current state-level policies in the United States, January 1, 2007-June 1, 2017, limiting high morphine equivalent daily dose (MEDD) prescribing.
Methods: State-level MEDD threshold policies were reviewed using LexisNexis and Westlaw Next for legislative acts and using Google for nonlegislative state-level policies. The websites of each state's Medicaid agency, health department, prescription drug monitoring program, workers' compensation board, medical board, and pharmacy board were reviewed to identify additional policies. The final policy list was checked against existing policy compilations and academic literature and through contact with state health agency representatives. Policies were independently double-coded on the categories: state, agency/organization, policy type, effective date, threshold level, and policy exceptions.
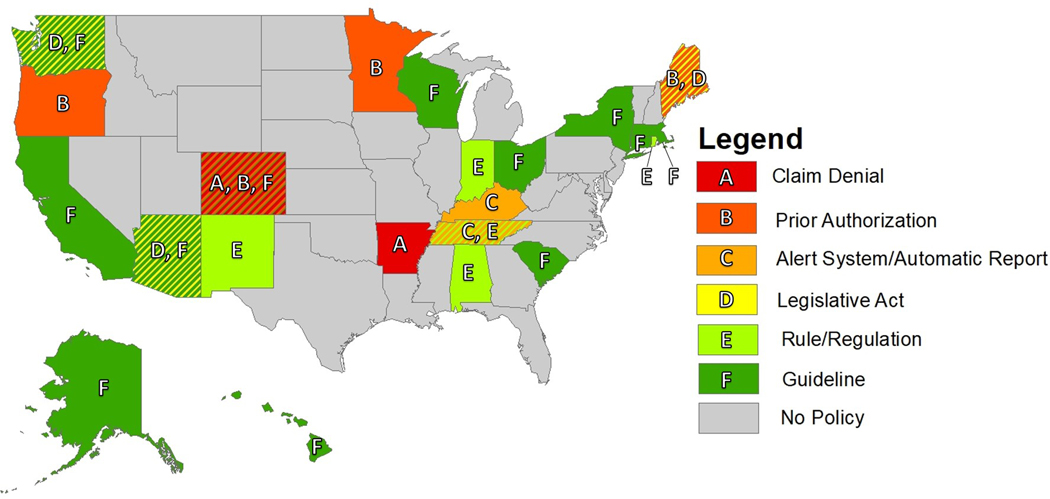
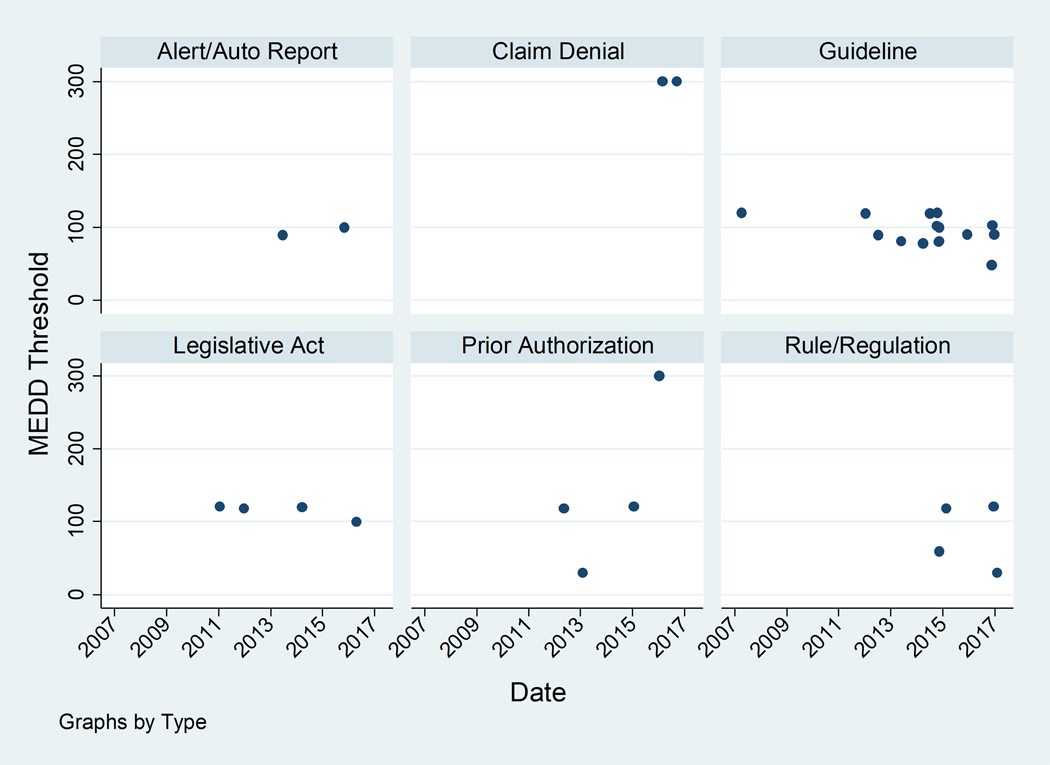
Results: Currently, 22 states have at least one type of MEDD policy, most commonly guidelines (14 states), followed by prior authorizations (four states), rules/regulations (four states), legislative acts (three states), claim denials (two states), and alert systems/automatic patient reports (two states). Thresholds range widely (30-300 mg MEDD), with higher thresholds generally corresponding to more restrictive policies (e.g., claim denial) and lower thresholds corresponding to less restrictive policies (e.g., guidelines). The majority of policies exclude some groups of opioid users, most commonly patients with terminal illnesses or acute pain.
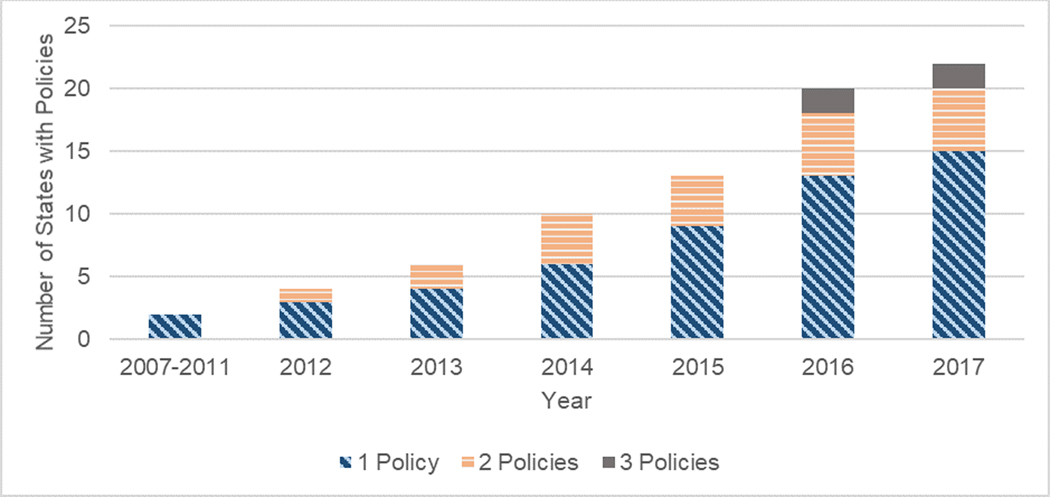
Conclusions: MEDD policies have gained popularity in recent years, but considerable variation in threshold levels and policy structure point to a lack of consensus. This work provides a foundation for future evaluation of MEDD policies and may inform states considering adopting such policies.
Keywords: Opioids; Prescriptions; Quality of Health Care.
© 2019 American Academy of Pain Medicine. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Conflict of Interest/Disclosure Summary
Dr. Alexander is Chair of FDA’s Peripheral and Central Nervous System Advisory Committee, has served as a paid advisor to IQVIA, serves on the advisory board of MesaRx Innovations, is a member of OptumRx’s National P&T Committee; and holds equity in Monument Analytics, a health care consultancy whose clients include the life sciences industry as well as plaintiffs in opioid litigation. This arrangement has been reviewed and approved by Johns Hopkins University in accordance with its conflict of interest policies. Drs. Frey and Castillo are employed by Johns Hopkins University and Dr. Heins is employed by RAND Corporation and have no conflicts of interest to disclose.
Figures
References
-
- Bohnert ASB, Valenstein M, Bair MJ, et al. Association between opioid prescribing patterns and opioid overdose-related deaths. JAMA J Am Med Assoc 2011;305(13):1315–1321. - PubMed
-
- Gomes T, Mamdani MM, Dhalla IA, Paterson JM, Juurlink DN. Opioid dose and drug-related mortality in patients with nonmalignant pain. Arch Intern Med 2011;171(7):686–691. - PubMed
