

Hypertension Associated with Fructose and High Salt: Renal and Sympathetic Mechanisms
- PMID: 30866441
- PMCID: PMC6472002
- DOI: 10.3390/nu11030569
Hypertension Associated with Fructose and High Salt: Renal and Sympathetic Mechanisms
Abstract
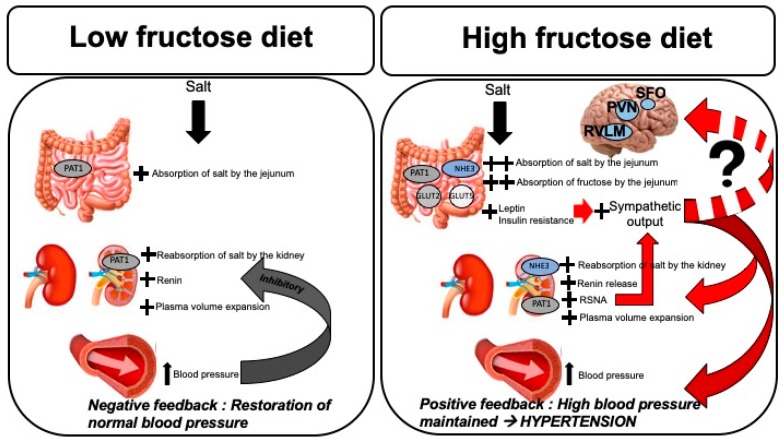
Hypertension is a leading cause of cardiovascular and chronic renal disease. Despite multiple important strides that have been made in our understanding of the etiology of hypertension, the mechanisms remain complex due to multiple factors, including the environment, heredity and diet. This review focuses on dietary contributions, providing evidence for the involvement of elevated fructose and salt consumption that parallels the increased incidence of hypertension worldwide. High fructose loads potentiate salt reabsorption by the kidney, leading to elevation in blood pressure. Several transporters, such as NHE3 and PAT1 are modulated in this milieu and play a crucial role in salt-sensitivity. High fructose ingestion also modulates the renin-angiotensin-aldosterone system. Recent attention has been shifted towards the contribution of the sympathetic nervous system, as clinical trials demonstrated significant reductions in blood pressure following renal sympathetic nerve ablation. New preclinical data demonstrates the activation of the renal sympathetic nerves in fructose-induced salt-sensitive hypertension, and reductions of blood pressure after renal nerve ablation. This review further demonstrates the interplay between sodium handling by the kidney, the renin-angiotensin-aldosterone system, and activation of the renal sympathetic nerves as important mechanisms in fructose and salt-induced hypertension.
Keywords: fructose; hypertension; renal sympathetic nerve activity; renal transporters; renin-angiotensin-aldosterone system; sodium.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Yano Y., Reis J.P., Colangelo L.A., Shimbo D., Viera A.J., Allen N.B., Gidding S.S., Bress A.P., Greenland P., Muntner P., et al. Association of Blood Pressure Classification in Young Adults Using the 2017 American College of Cardiology/American Heart Association Blood Pressure Guideline with Cardiovascular Events Later in Life. JAMA. 2018;320:1774–1782. doi: 10.1001/jama.2018.13551. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
