

Microscopic versus endoscopic transsphenoidal surgery in the Leiden cohort treated for Cushing's disease: surgical outcome, mortality, and complications
- PMID: 30866993
- PMCID: PMC6416951
- DOI: 10.1186/s13023-019-1038-0
Microscopic versus endoscopic transsphenoidal surgery in the Leiden cohort treated for Cushing's disease: surgical outcome, mortality, and complications
Abstract
Background: First-choice treatment for Cushing's disease is transsphenoidal adenomectomy. Since its introduction in the 1970s, many centers have now switched from microscopic to endoscopic surgery. We compared both techniques for the treatment of Cushing's disease at the Leiden University Medical Center, a European reference center for pituitary diseases.
Methods: Cohort study with inclusion and follow-up of consecutive Cushing's disease patients primarily treated by transsphenoidal surgery at the Leiden University Medical Center between 1978 and 2016. We compared remission rates (primary endpoint), mortality, and complications between microscopic (performed up to 2005) and endoscopic (performed from 2003 onwards) surgery. Subgroup analyses were performed by tumor size, surgical experience, and preoperative imaging techniques. Additionally, surgeons' intraoperative findings regarding presence and removal of the adenoma were related to surgical outcome.
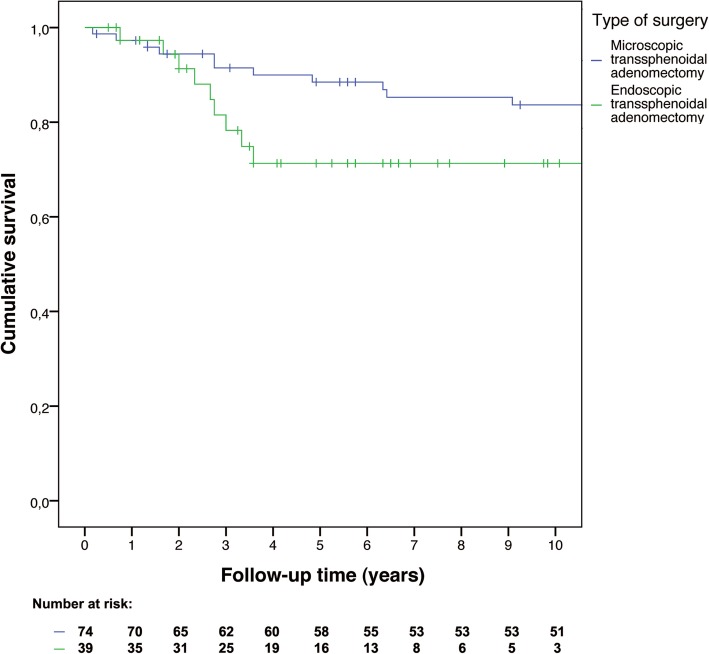
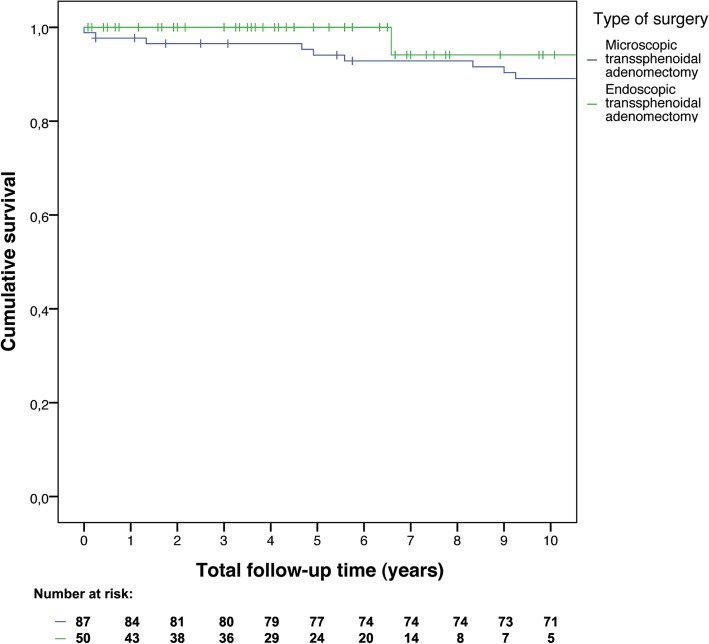
Results: Of 137 included patients, 87 were treated microscopically and 50 endoscopically. Three months after microscopic surgery, 74 patients (86%) were in remission. Five-year recurrence-free survival was 89% (95% confidence interval [CI]: 82-96%), and ten-year recurrence free survival was 84% (95% CI: 75-93%). After endoscopic surgery, 39 patients (83%) were in remission. Both five-year and ten-year recurrence-free survival were 71% (95% CI: 55-87%). Hazard ratio for recurrence was 0.47 (95% CI: 0.19-1.14), and for mortality 2.79 (95% CI: 0.35-22.51), for microscopic versus endoscopic surgery. No learning curve was found for endoscopy, nor an influence of preoperative imaging technique for microscopy. In addition, we did not find a clear relation between the surgeons' intraoperative findings and surgical outcomes.
Conclusions: This study did not identify a clear advantage of microscopic or endoscopic transsphenoidal surgery for the treatment of Cushing's disease based on clinical outcome. The transition to endoscopic surgery at our center was not accompanied by transient worsening of outcomes, which may be reassuring for those considering transitioning.
Keywords: Complications; Cushing’s disease; Endoscopy; Microscopy; Surgical outcome; Transsphenoidal adenomectomy.
Conflict of interest statement
Ethics approval and consent to participate
Patients gave informed consent to use their data for scientific research. Permission from the ethical committee (MEC) in the LUMC was granted.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures





References
-
- Lindholm J, Juul S, Jorgensen JO, Astrup J, Bjerre P, Feldt-Rasmussen U, et al. Incidence and late prognosis of cushing's syndrome: a population-based study. J Clin Endocrinol Metab. 2001;86(1):117–123. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
