

Joint association of urinary sodium and potassium excretion with cardiovascular events and mortality: prospective cohort study
- PMID: 30867146
- PMCID: PMC6415648
- DOI: 10.1136/bmj.l772
Joint association of urinary sodium and potassium excretion with cardiovascular events and mortality: prospective cohort study
Abstract
Objective: To evaluate the joint association of sodium and potassium urinary excretion (as surrogate measures of intake) with cardiovascular events and mortality, in the context of current World Health Organization recommendations for daily intake (<2.0 g sodium, >3.5 g potassium) in adults.
Design: International prospective cohort study.
Setting: 18 high, middle, and low income countries, sampled from urban and rural communities.
Participants: 103 570 people who provided morning fasting urine samples.
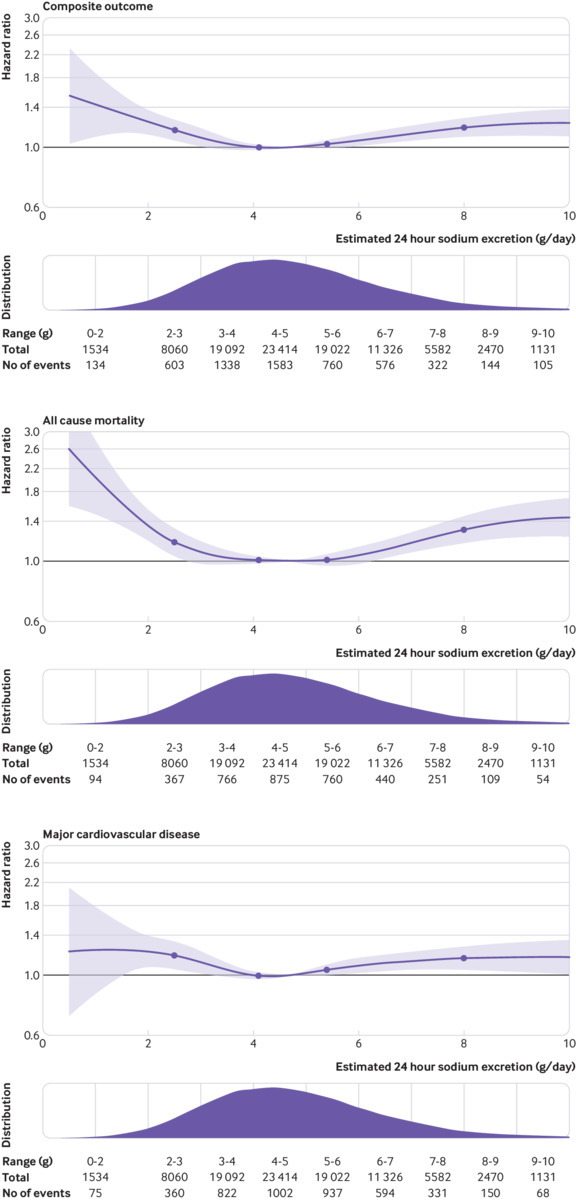
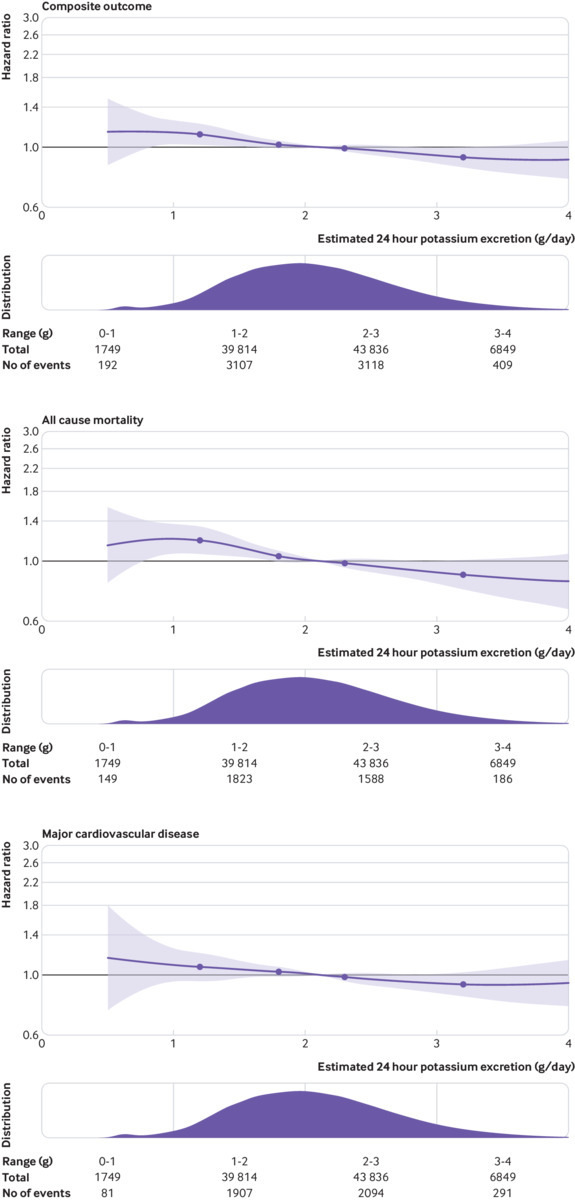
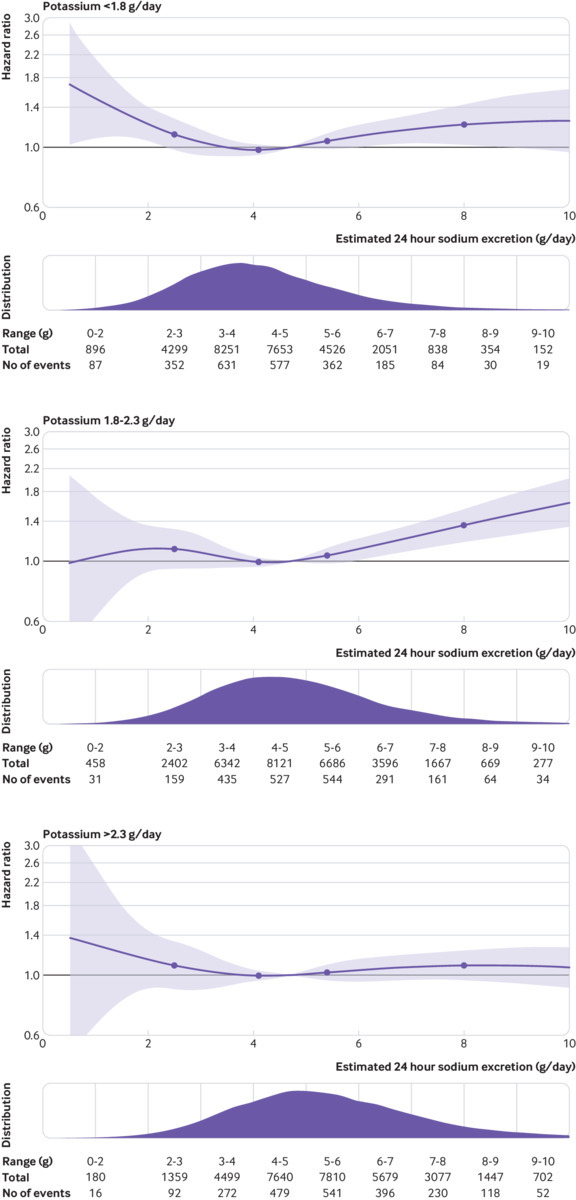
Main outcome measures: Association of estimated 24 hour urinary sodium and potassium excretion (surrogates for intake) with all cause mortality and major cardiovascular events, using multivariable Cox regression. A six category variable for joint sodium and potassium was generated: sodium excretion (low (<3 g/day), moderate (3-5 g/day), and high (>5 g/day) sodium intakes) by potassium excretion (greater/equal or less than median 2.1 g/day).
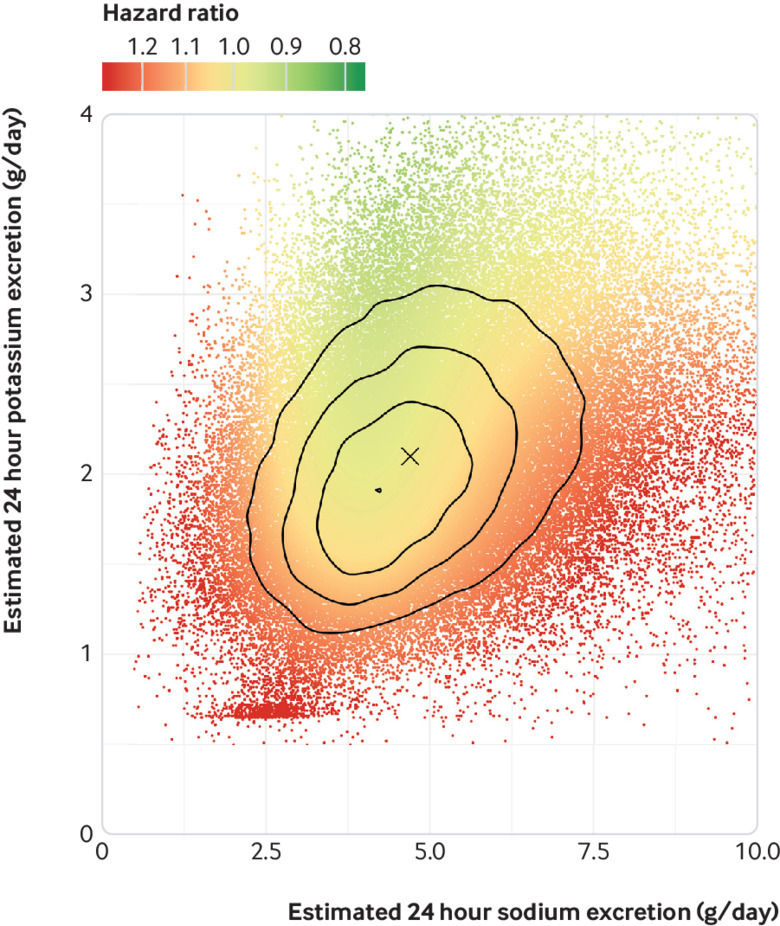
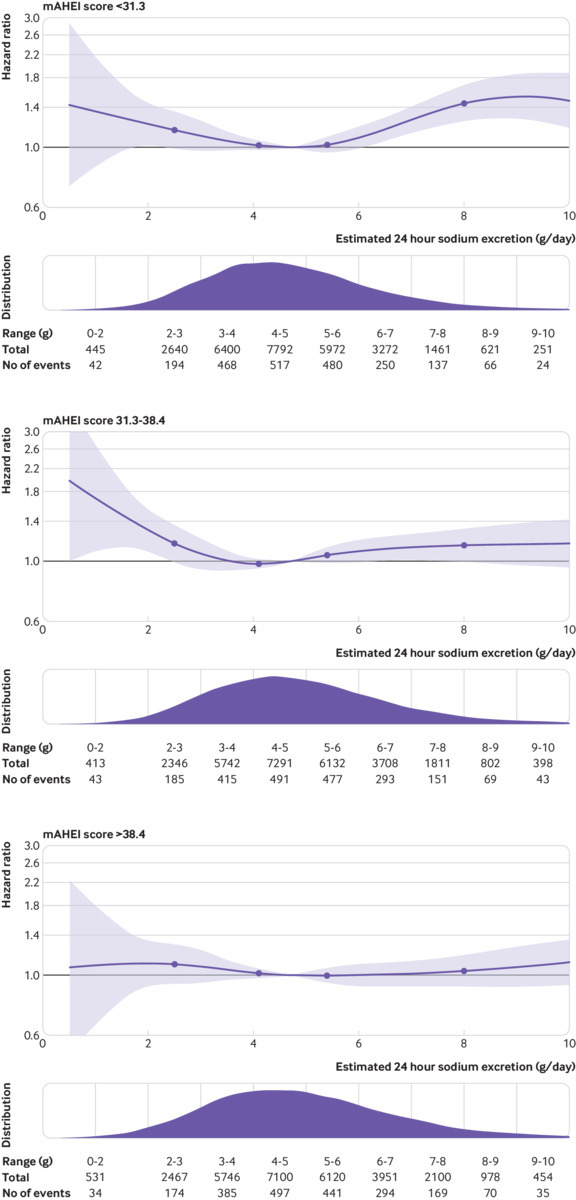
Results: Mean estimated sodium and potassium urinary excretion were 4.93 g/day and 2.12 g/day, respectively. After a median follow-up of 8.2 years, 7884 (6.1%) participants had died or experienced a major cardiovascular event. Increasing urinary sodium excretion was positively associated with increasing potassium excretion (unadjusted r=0.34), and only 0.002% had a concomitant urinary excretion of <2.0 g/day of sodium and >3.5 g/day of potassium. A J-shaped association was observed of sodium excretion and inverse association of potassium excretion with death and cardiovascular events. For joint sodium and potassium excretion categories, the lowest risk of death and cardiovascular events occurred in the group with moderate sodium excretion (3-5 g/day) and higher potassium excretion (21.9% of cohort). Compared with this reference group, the combinations of low potassium with low sodium excretion (hazard ratio 1.23, 1.11 to 1.37; 7.4% of cohort) and low potassium with high sodium excretion (1.21, 1.11 to 1.32; 13.8% of cohort) were associated with the highest risk, followed by low sodium excretion (1.19, 1.02 to 1.38; 3.3% of cohort) and high sodium excretion (1.10, 1.02 to 1.18; 29.6% of cohort) among those with potassium excretion greater than the median. Higher potassium excretion attenuated the increased cardiovascular risk associated with high sodium excretion (P for interaction=0.007).
Conclusions: These findings suggest that the simultaneous target of low sodium intake (<2 g/day) with high potassium intake (>3.5 g/day) is extremely uncommon. Combined moderate sodium intake (3-5 g/day) with high potassium intake is associated with the lowest risk of mortality and cardiovascular events.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any additional organisation for the submitted work. A detailed list of funders is provided in the supplementary appendix. The authors have no financial relationships with any organisations, or other relationships or activities, that might have influenced the submitted work in the previous three years.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical