

Host tissue determinants of tumour immunity
- PMID: 30867580
- PMCID: PMC7787168
- DOI: 10.1038/s41568-019-0125-9
Host tissue determinants of tumour immunity
Abstract
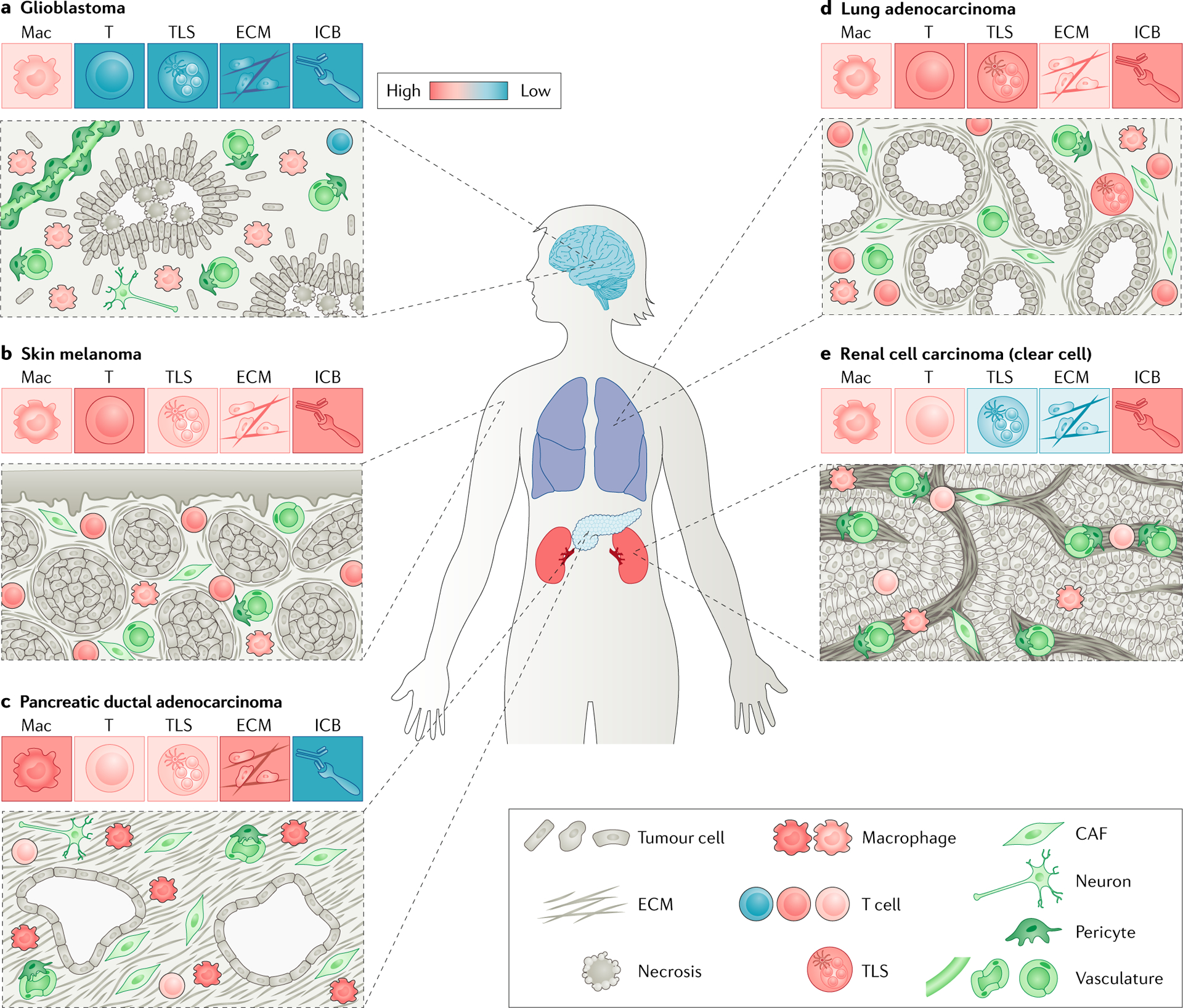
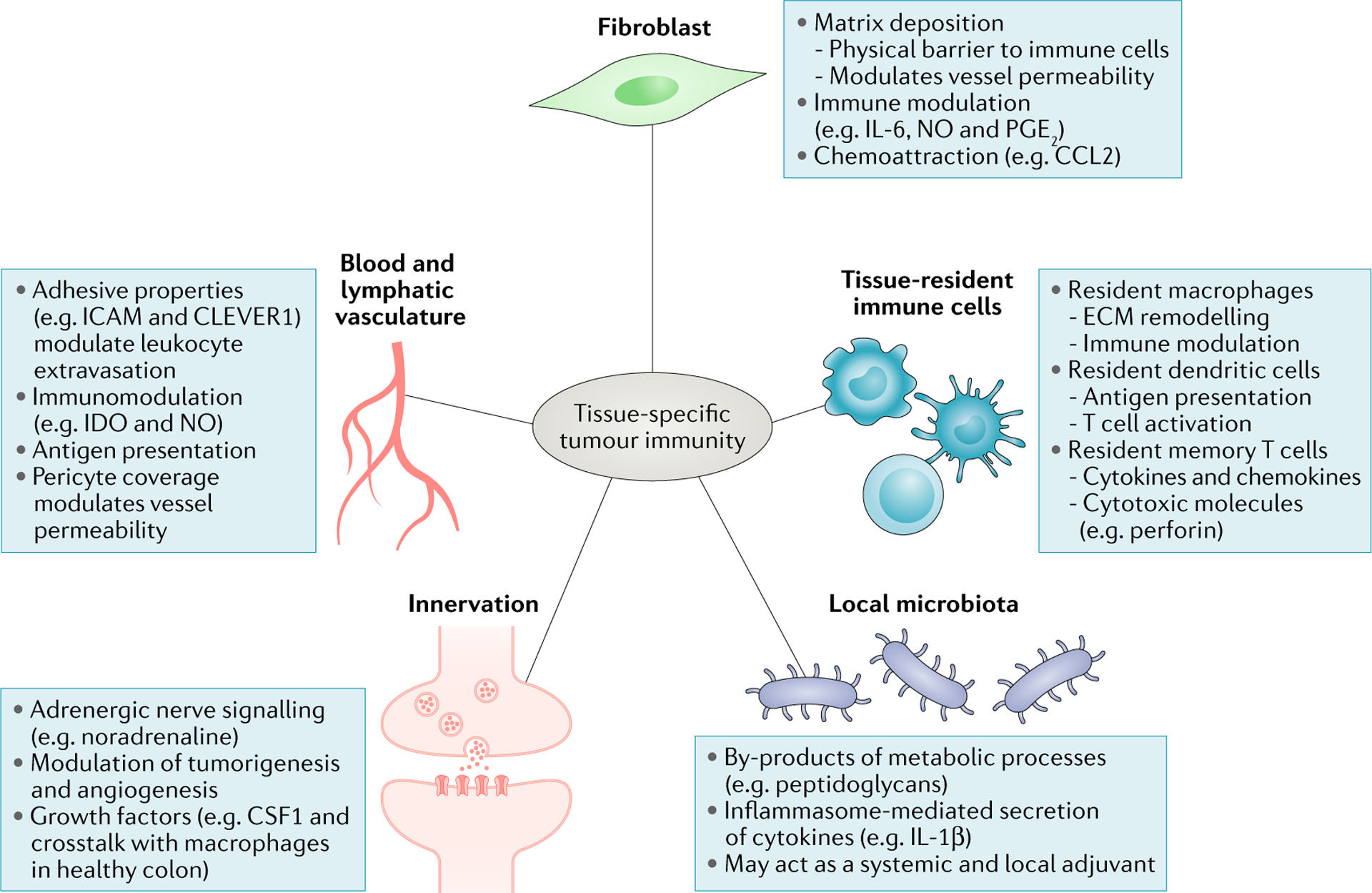
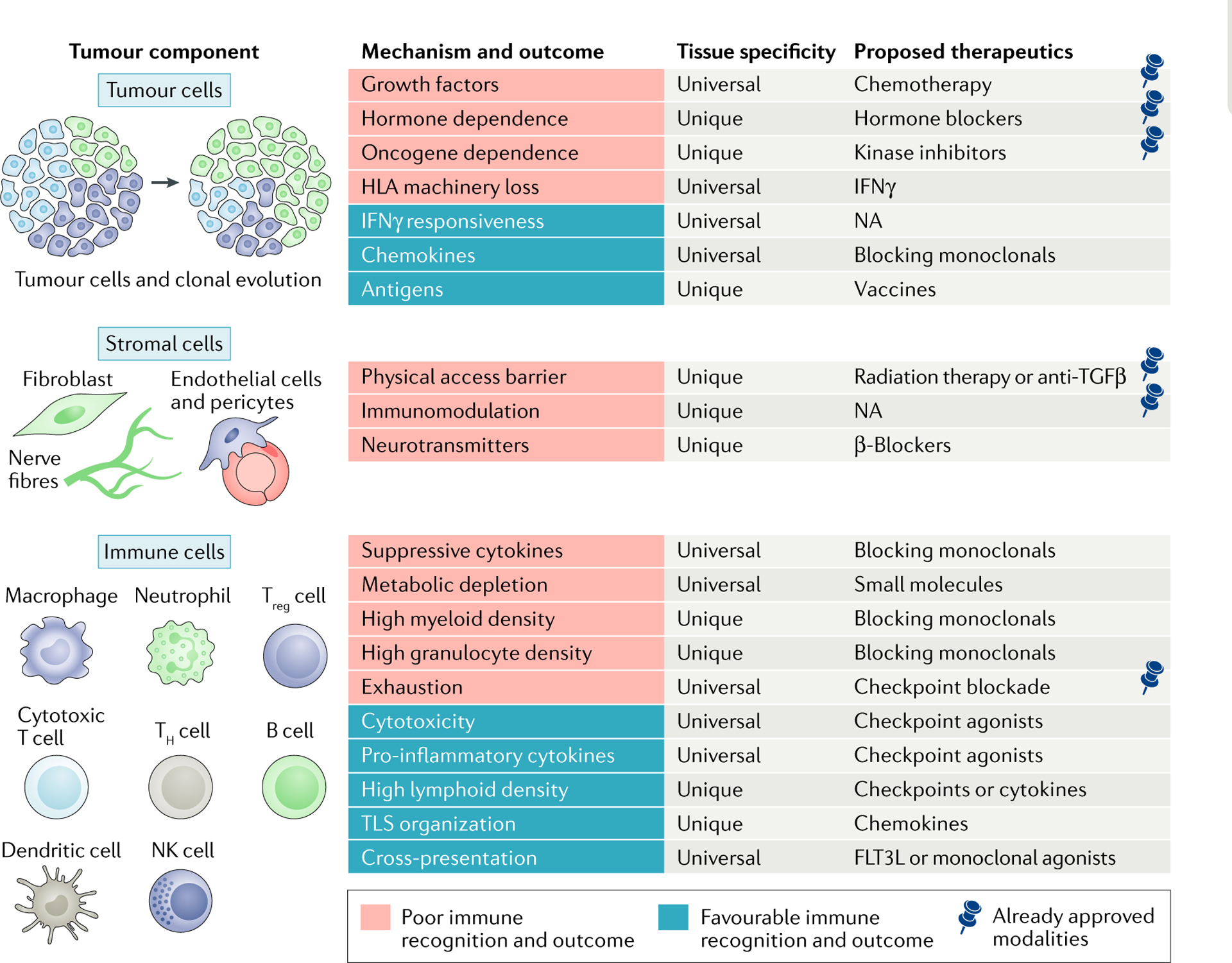
Although common evolutionary principles drive the growth of cancer cells regardless of the tissue of origin, the microenvironment in which tumours arise substantially differs across various organ sites. Recent studies have established that, in addition to cell-intrinsic effects, tumour growth regulation also depends on local cues driven by tissue environmental factors. In this Review, we discuss how tissue-specific determinants might influence tumour development and argue that unravelling the tissue-specific contribution to tumour immunity should help the development of precise immunotherapeutic strategies for patients with cancer.
Conflict of interest statement
Competing interests
H.S. receives research funding from Takeda and Genentech. R.R. is an employee of Innate Pharma. S.G. reports consultancy and/or advisory roles for Merck, Neon Therapeutics and OncoMed and research funding from Bristol-Myers Squibb, Genentech, Immune Design, Agenus, Janssen R&D and Pfizer. M.M. receives funding from Regeneron, Takeda, Genentech and Boehringer Ingelheim.
Figures
References
Publication types
MeSH terms
Grants and funding
- R01 CA154947 /NH/NIH HHS/United States
- U19 AI128949/AI/NIAID NIH HHS/United States
- R01 CA190400 /NH/NIH HHS/United States
- U19 AI128949 /NH/NIH HHS/United States
- R01 AI113221 /NH/NIH HHS/United States
- U19 AI117873 /NH/NIH HHS/United States
- R01 CA190400/CA/NCI NIH HHS/United States
- P01 CA190174/CA/NCI NIH HHS/United States
- U19 AI117873/AI/NIAID NIH HHS/United States
- R01 CA224319 /NH/NIH HHS/United States
- U24 AI118644 /NH/NIH HHS/United States
- U24 AI118644/AI/NIAID NIH HHS/United States
- R01 AI113221/AI/NIAID NIH HHS/United States
- U24 CA224319/CA/NCI NIH HHS/United States
- R01 CA154947/CA/NCI NIH HHS/United States
- CA190174 /NH/NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
