

Medicare expenditures attributable to dementia
- PMID: 30868557
- PMCID: PMC6606539
- DOI: 10.1111/1475-6773.13134
Medicare expenditures attributable to dementia
Abstract
Objective: To estimate dementia's incremental cost to the traditional Medicare program.
Data sources: Health and Retirement Study (HRS) survey-linked Medicare part A and B claims from 1991 to 2012.
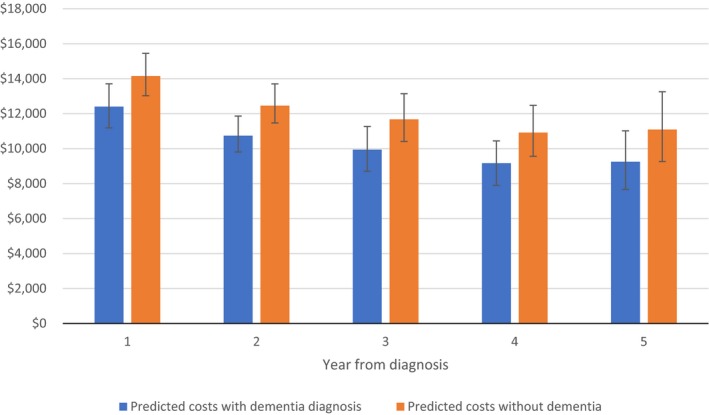
Study design: We compared Medicare expenditures for 60 months following a claims-based dementia diagnosis to those for a randomly selected, matched comparison group.
Data collection/extraction methods: We used a cost estimator that accounts for differential survival between individuals with and without dementia and decomposes incremental costs into survival and cost intensity components.
Principal findings: Dementia's five-year incremental cost to the traditional Medicare program is approximately $15 700 per patient, nearly half of which is incurred in the first year after diagnosis. Shorter survival with dementia mitigates the incremental cost by about $2650. Increased costs for individuals with dementia were driven by more intensive use of Medicare part A covered services. The incremental cost of dementia was about $7850 higher for females than for males because of sex-specific differential mortality associated with dementia.
Conclusions: Dementia's cost to the traditional Medicare program is significant. Interventions that target early identification of dementia and preventable inpatient and post-acute care services could produce substantial savings.
Keywords: Alzheimer's disease; Medicare; aging; dementia; health care costs.
© Health Research and Educational Trust.
Conflict of interest statement
Lindsay White, Paul Fishman, Anirban Basu, Paul Crane, Eric Larson, and Norma Coe declare that they have no conflicts of interest.
Figures
References
-
- Alzheimer's Association . What is dementia? 2016. http://www.alz.org/what-is-dementia.asp. Accessed November 5, 2016.
-
- Prince M, Bryce R, Albanese E, Wimo A, Ribeiro W, Ferri CP. The global prevalence of dementia: a systematic review and metaanalysis. Alzheimers Dement. 2013;9(1):63‐75 e62. - PubMed
-
- Bynum JP, Rabins PV, Weller W, Niefeld M, Anderson GF, Wu AW. The relationship between a dementia diagnosis, chronic illness, medicare expenditures, and hospital use. J Am Geriatr Soc. 2004;52(2):187‐194. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
