

Association of Surgical and Hospital Volume and Patient Characteristics With 30-Day Readmission Rates
- PMID: 30869738
- PMCID: PMC6481432
- DOI: 10.1001/jamaoto.2018.4504
Association of Surgical and Hospital Volume and Patient Characteristics With 30-Day Readmission Rates
Abstract
Importance: Thirty-day readmission rates have been suggested as a marker for quality of care. By investigating the factors associated with readmissions in all otolaryngology subspecialties we provide data relevant for the development of risk stratification systems to improve outcomes.
Objective: To establish the association of surgical and hospital volume and patient characteristics with 30-day readmission rates to guide the development of otolaryngology-specific risk stratification models.
Design, setting, and participants: A retrospective cohort study including adult patients who underwent inpatient otolaryngology surgery in New York State between 1995 and 2015 was conducted using the Statewide Planning and Research Cooperative System (SPARCS). Regression techniques were used to describe relationships of patient-level factors, hospital, and surgeon volume to 30-day readmission rates in New York State.
Main outcomes and measures: The main outcome measures were patient-, surgeon-, and hospital-level risk factors for readmission. Secondary outcome measures were rate of readmissions by subspecialty procedure and by diagnosis on readmission.
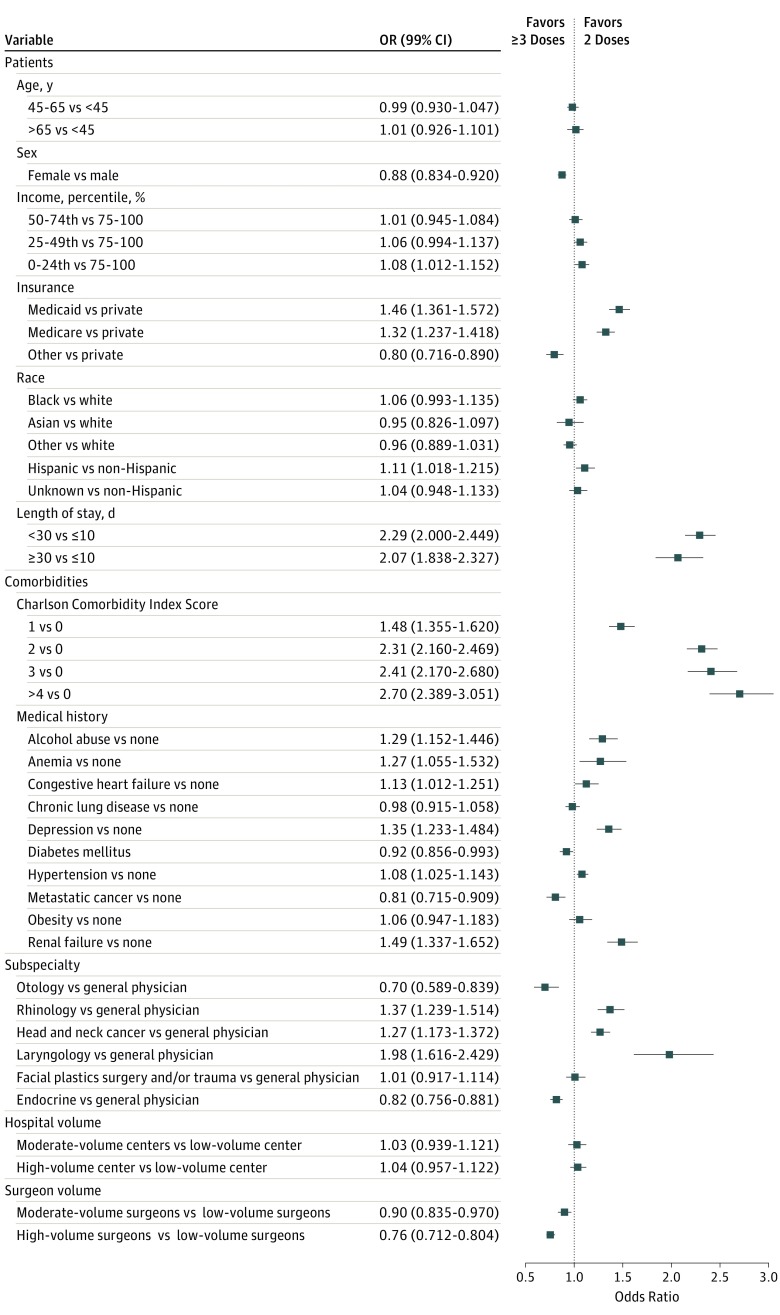
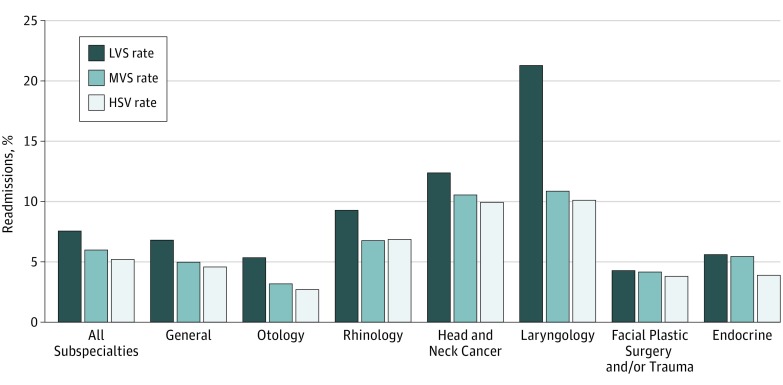
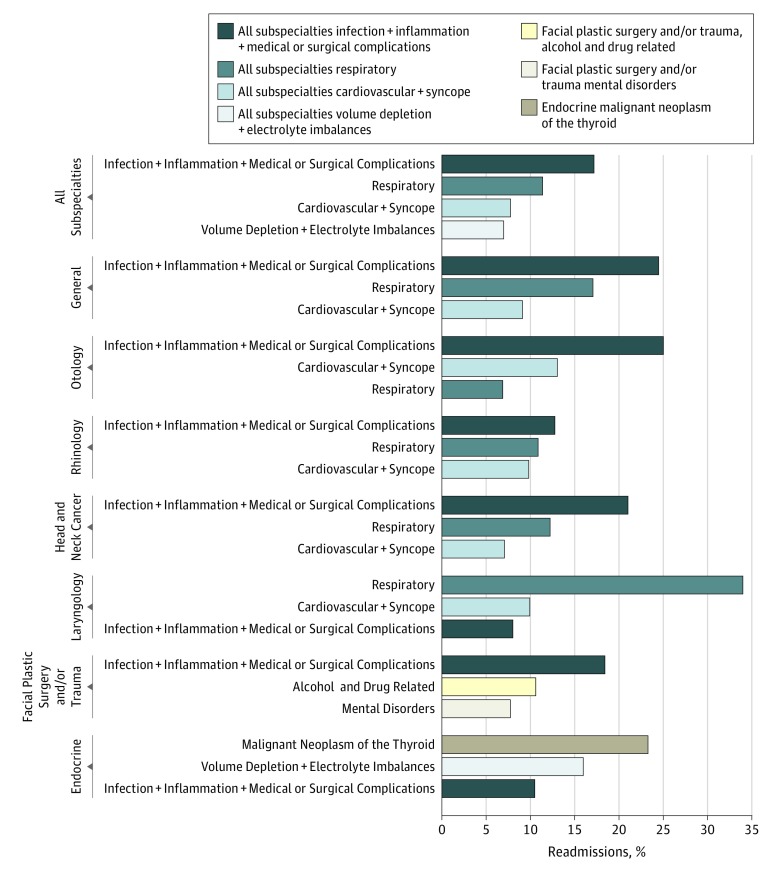
Results: We identified 254 257 cases of otolaryngology surgery (147 065 women [58%], mean [SD] age 50 [17] years). The 30-day readmission rate was 6%. In a multivariable model, odds ratios (ORs) identified Medicaid insurance (OR, 1.46; 99% CI, 1.36-1.57), Medicare insurance (OR, 1.32; 99% CI, 1.24-1.42), bottom quartile income (OR, 1.08; 99% CI, 1.01-1.15), patient comorbidities measured by the Charlson Comorbidity Index (CCI) (CCI >1; OR, 2.31; 99% CI, 2.16-2.47), length of stay (LOS) (LOS >10 days; OR, 2.29; 99% CI, 2.00-2.45), rhinology (OR, 1.37; 99% CI, 1.24-1.51), laryngology (OR, 1.98; 99% CI, 1.62-2.43), and head and neck cancer (OR, 1.27; 99% CI, 1.17-1.37) procedures as readmission predictors. High-volume surgeons were protective of 30-day readmission (OR, 0.67; 99% CI, 0.635-0.708) relative to low volume. Hospital volume was not significantly associated to readmissions. The most common causes of readmission included wound- (2682 patients, 18%), respiratory- (1776 patients, 12%), cardiovascular- (1210 patients, 8%), and volume- (1089 patients, 7%) related disorders.
Conclusions and relevance: This study evaluated the combined effects of patient-, surgeon-, and hospital-level factors on 30-day readmission after otolaryngology surgery. Socioeconomic factors, patient comorbidities, surgeon volumes, and procedure were significantly associated with 30-day readmission. Though the cause of 30-day readmission is multifactorial, a large portion is driven by socioeconomic factors. Addressing these disparities at the system level is necessary to address the described readmission disparities. The development of risk-stratification models based on patient-, procedure-, and surgeon-level factors may help facilitate resource distribution.
Conflict of interest statement
Figures
Comment in
-
Risk Factors for 30-Day Readmission of Otolaryngology Patients.JAMA Otolaryngol Head Neck Surg. 2019 Apr 1;145(4):337-338. doi: 10.1001/jamaoto.2019.0005. JAMA Otolaryngol Head Neck Surg. 2019. PMID: 30869768 No abstract available.
References
-
- Services CfMaM Readmissions Reduction Program (HRRP). 2018; https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpat.... Accessed March 1, 2018.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
