

Identifying Women at High Risk for Breast Cancer Using Data From the Electronic Health Record Compared With Self-Report
- PMID: 30869999
- PMCID: PMC6874029
- DOI: 10.1200/CCI.18.00072
Identifying Women at High Risk for Breast Cancer Using Data From the Electronic Health Record Compared With Self-Report
Abstract
Purpose: A barrier to chemoprevention uptake among high-risk women is the lack of routine breast cancer risk assessment in the primary care setting. We calculated breast cancer risk using the Breast Cancer Surveillance Consortium (BCSC) model, accounting for age, race/ethnicity, first-degree family history of breast cancer, benign breast disease, and mammographic density, using data collected from the electronic health records (EHRs) and self-reports.
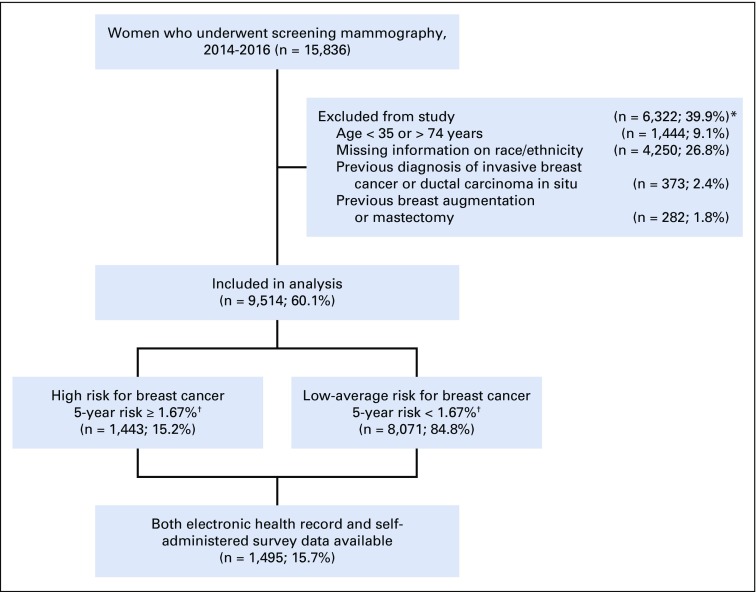
Patients and methods: Among women undergoing screening mammography, we enrolled those age 35 to 74 years without a prior history of breast cancer. Data on demographics, first-degree family history, breast radiology, and pathology reports were extracted from the EHR. We assessed agreement between the EHR and self-report on information about breast cancer risk.
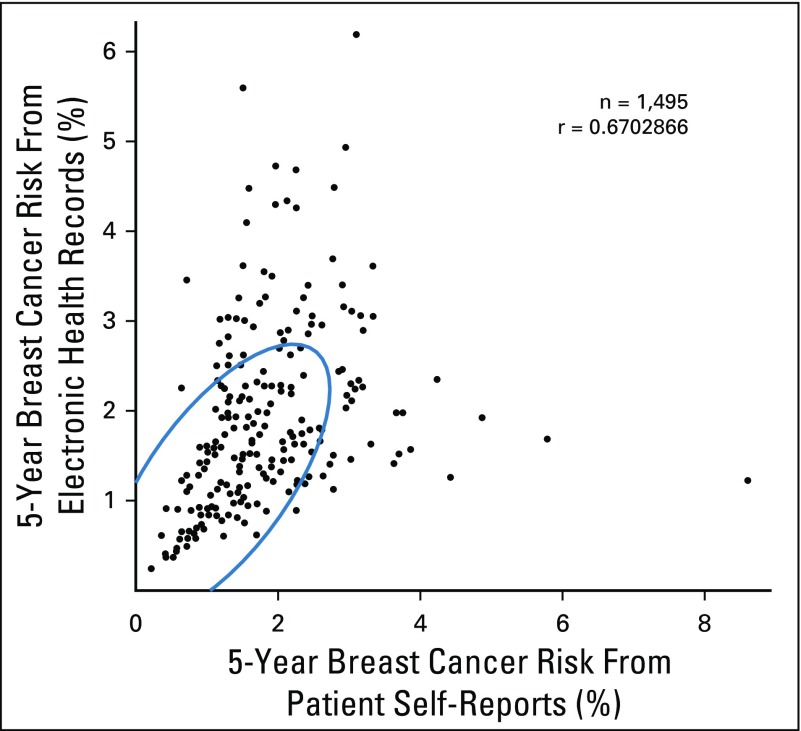
Results: Among 9,514 women with known race/ethnicity, 1,443 women (15.2%) met high-risk criteria based upon a 5-year invasive breast cancer risk of 1.67% or greater according to the BCSC model. Among 1,495 women with both self-report and EHR data, more women with a first-degree family history of breast cancer (14.6% v 4.4%) and previous breast biopsies (21.3% v 11.3%) were identified by self-report versus EHR, respectively. However, more women with atypia and lobular carcinoma in situ were identified from the EHR. There was moderate agreement in identification of high-risk women between EHR and self-report data (κ, 0.48; 95% CI, 0.42-0.54).
Conclusion: By using EHR data, we determined that 15% of women undergoing screening mammography had a high risk for breast cancer according to the BCSC model. There was moderate agreement between information on breast cancer risk derived from the EHR and self-report. Examining EHR data may serve as an initial screen for identifying women eligible for breast cancer chemoprevention.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
No potential conflicts of interest were reported.
Figures
Similar articles
-
Assessing breast cancer risk within the general screening population: developing a breast cancer risk model to identify higher risk women at mammographic screening.Eur Radiol. 2020 Oct;30(10):5417-5426. doi: 10.1007/s00330-020-06901-x. Epub 2020 May 1. Eur Radiol. 2020. PMID: 32358648
-
Breast Density and Benign Breast Disease: Risk Assessment to Identify Women at High Risk of Breast Cancer.J Clin Oncol. 2015 Oct 1;33(28):3137-43. doi: 10.1200/JCO.2015.60.8869. Epub 2015 Aug 17. J Clin Oncol. 2015. PMID: 26282663 Free PMC article.
-
Validation of self-reported post-treatment mammography surveillance among breast cancer survivors by electronic medical record extraction method.Breast Cancer Res Treat. 2015 Jun;151(2):427-34. doi: 10.1007/s10549-015-3387-2. Epub 2015 Apr 29. Breast Cancer Res Treat. 2015. PMID: 25922083 Free PMC article.
-
Epidemiology, genetics, and risk evaluation of postmenopausal women at risk of breast cancer.Menopause. 2008 Jul-Aug;15(4 Suppl):782-9. doi: 10.1097/gme.0b013e3181788d88. Menopause. 2008. PMID: 18596599 Review.
-
Management of Women at High Risk for Breast Cancer.J Am Board Fam Med. 2024 Jan 5;36(6):1029-1032. doi: 10.3122/jabfm.2023.230064R1. J Am Board Fam Med. 2024. PMID: 37857439 Review.
Cited by
-
Mental Illness and BRCA1/2 Genetic Testing Intention Among Multiethnic Women Undergoing Screening Mammography.Oncol Nurs Forum. 2020 Jan 1;47(1):E13-E24. doi: 10.1188/20.ONF.E13-E24. Oncol Nurs Forum. 2020. PMID: 31845917 Free PMC article.
-
Genetic counseling and testing for females at elevated risk for breast cancer: Protocol for the randomized controlled trial of the Know Your Risk intervention.Contemp Clin Trials. 2023 Oct;133:107323. doi: 10.1016/j.cct.2023.107323. Epub 2023 Sep 1. Contemp Clin Trials. 2023. PMID: 37661005 Free PMC article.
-
Risk-management decision-making data from a community-based sample of racially diverse women at high risk of breast cancer: rationale, methods, and sample characteristics of the Daughter Sister Mother Project survey.Breast Cancer Res. 2024 Jan 11;26(1):8. doi: 10.1186/s13058-023-01753-x. Breast Cancer Res. 2024. PMID: 38212792 Free PMC article.
-
Extraction of Electronic Health Record Data using Fast Healthcare Interoperability Resources for Automated Breast Cancer Risk Assessment.AMIA Annu Symp Proc. 2022 Feb 21;2021:843-852. eCollection 2021. AMIA Annu Symp Proc. 2022. PMID: 35308910 Free PMC article.
-
User Comprehension and EHR Integration of the RealRisks Decision Aid for Breast Cancer Risk Assessment: A Qualitative Study.AMIA Annu Symp Proc. 2025 May 22;2024:1129-1138. eCollection 2024. AMIA Annu Symp Proc. 2025. PMID: 40417528 Free PMC article.
References
-
- National Cancer Institute, Surveillance, Epidemiology, and End Results (SEER) Cancer Stat Facts: Female Breast Cancer. 2017 https://seer.cancer.gov/statfacts/html/breast.html
-
- Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for the prevention of breast cancer: Current status of the National Surgical Adjuvant Breast and Bowel Project P-1 study. J Natl Cancer Inst. 2005;97:1652–1662. - PubMed
-
- Cuzick J, Sestak I, Forbes JF, et al. Anastrozole for prevention of breast cancer in high-risk postmenopausal women (IBIS-II): An international, double-blind, randomised placebo-controlled trial. Lancet. 2014;383:1041–1048. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
