

A generalizable method for estimating duration of HIV infections using clinical testing history and HIV test results
- PMID: 30870196
- PMCID: PMC6561657
- DOI: 10.1097/QAD.0000000000002190
A generalizable method for estimating duration of HIV infections using clinical testing history and HIV test results
Abstract
Objective: To determine the precision of new and established methods for estimating duration of HIV infection.
Design: A retrospective analysis of HIV testing results from serial samples in commercially available panels, taking advantage of extensive testing previously conducted on 53 seroconverters.
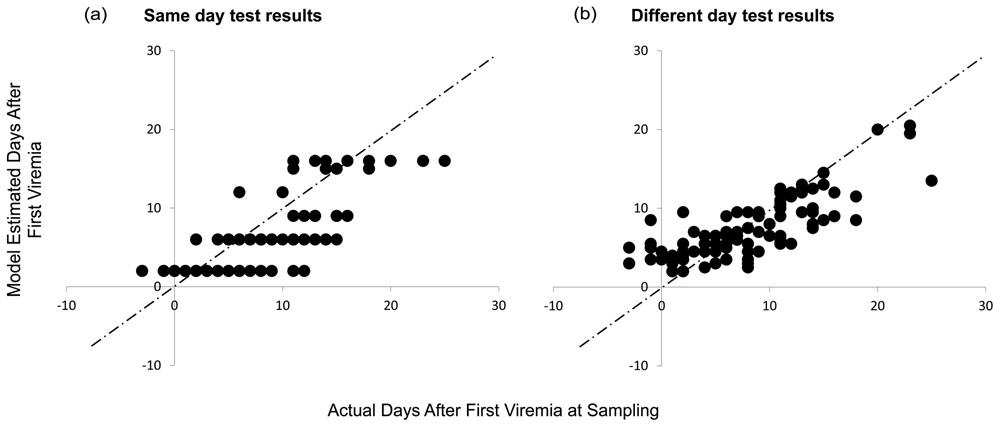
Methods: We initially investigated four methods for estimating infection timing: method 1, 'Fiebig stages' based on test results from a single specimen; method 2, an updated '4th gen' method similar to Fiebig stages but using antigen/antibody tests in place of the p24 antigen test; method 3, modeling of 'viral ramp-up' dynamics using quantitative HIV-1 viral load data from antibody-negative specimens; and method 4, using detailed clinical testing history to define a plausible interval and best estimate of infection time. We then investigated a 'two-step method' using data from both methods 3 and 4, allowing for test results to have come from specimens collected on different days.
Results: Fiebig and '4th gen' staging method estimates of time since detectable viremia had similar and modest correlation with observed data. Correlation of estimates from both new methods (3 and 4), and from a combination of these two ('two-step method') was markedly improved and variability significantly reduced when compared with Fiebig estimates on the same specimens.
Conclusion: The new 'two-step' method more accurately estimates timing of infection and is intended to be generalizable to more situations in clinical medicine, research, and surveillance than previous methods. An online tool is now available that enables researchers/clinicians to input data related to method 4, and generate estimated dates of detectable infection.
Figures


References
-
- Fiebig EW, Wright DJ, Rawal BD, Garrett PE, Schumacher RT, Peddada L, et al. Dynamics of HIV viremia and antibody seroconversion in plasma donors: implications for diagnosis and staging of primary HIV infection. AIDS. 2003;17(13):1871–9. - PubMed
-
- Cohen MS, Gay CL, Busch MP, Hecht FM. The detection of acute HIV infection. The Journal of Infectious Diseases. 2010;202 Suppl 2:S270–7. - PubMed
-
- Panel on Treatment of Pregnant Women with HIV Infection and Prevention of Perinatal Transmission. Recommendations for Use of Antiretroviral Drugs in Transmission in the United States; 2018.
-
- Priddy FH, Pilcher CD, Moore RH, Tambe P, Park MN, Fiscus SA, et al. Detection of acute HIV infections in an urban HIV counseling and testing population in the United States. Journal of Acquired Immune Deficiency Syndromes. 2007;44(2):196–202. - PubMed
